

Outcomes of surgery for giant hepatic hemangioma
- PMID: 33832476
- PMCID: PMC8033692
- DOI: 10.1186/s12893-021-01185-4
Outcomes of surgery for giant hepatic hemangioma
Abstract
Background: The surgical indications for liver hemangioma remain unclear.
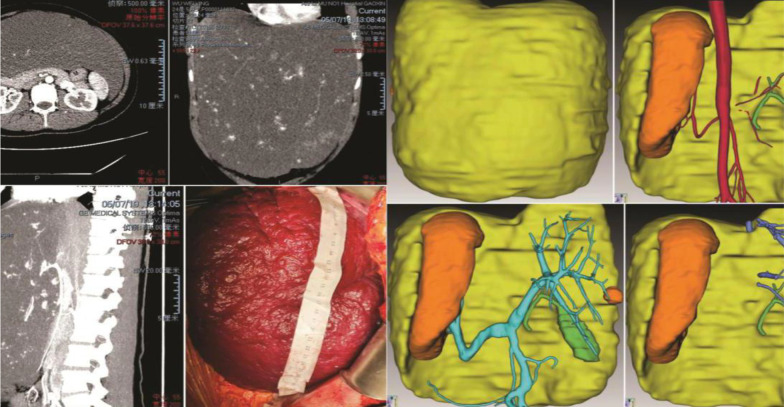
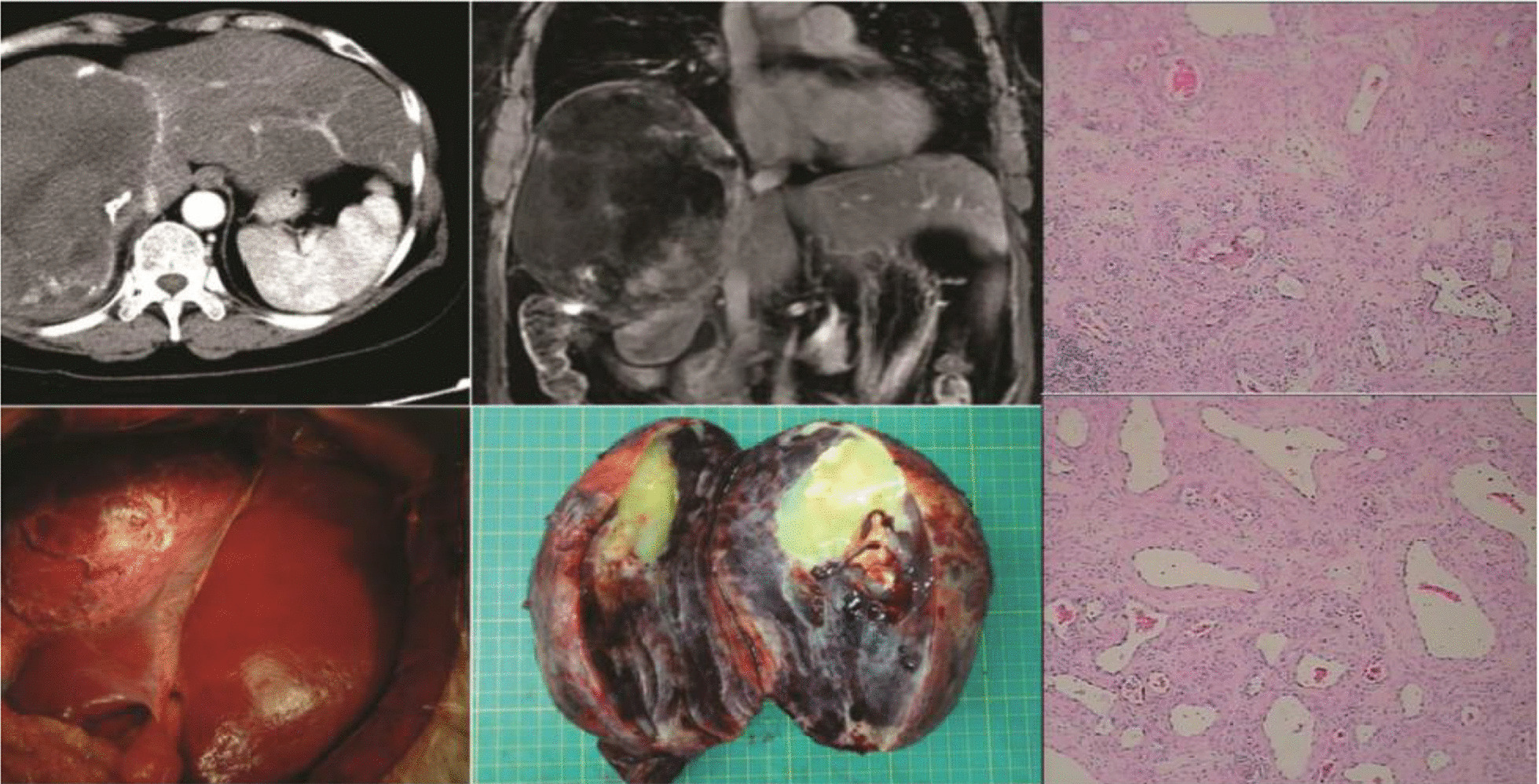
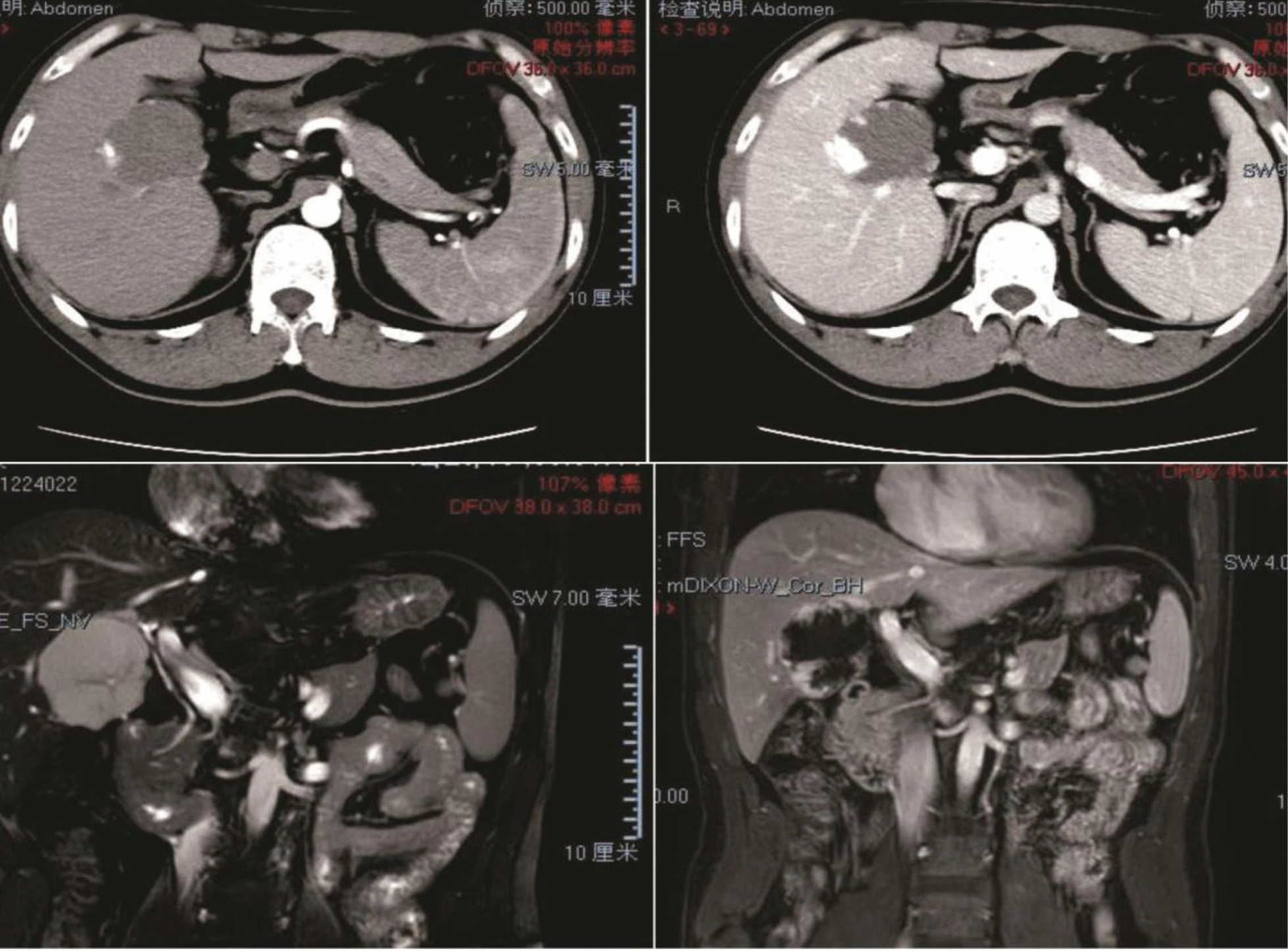
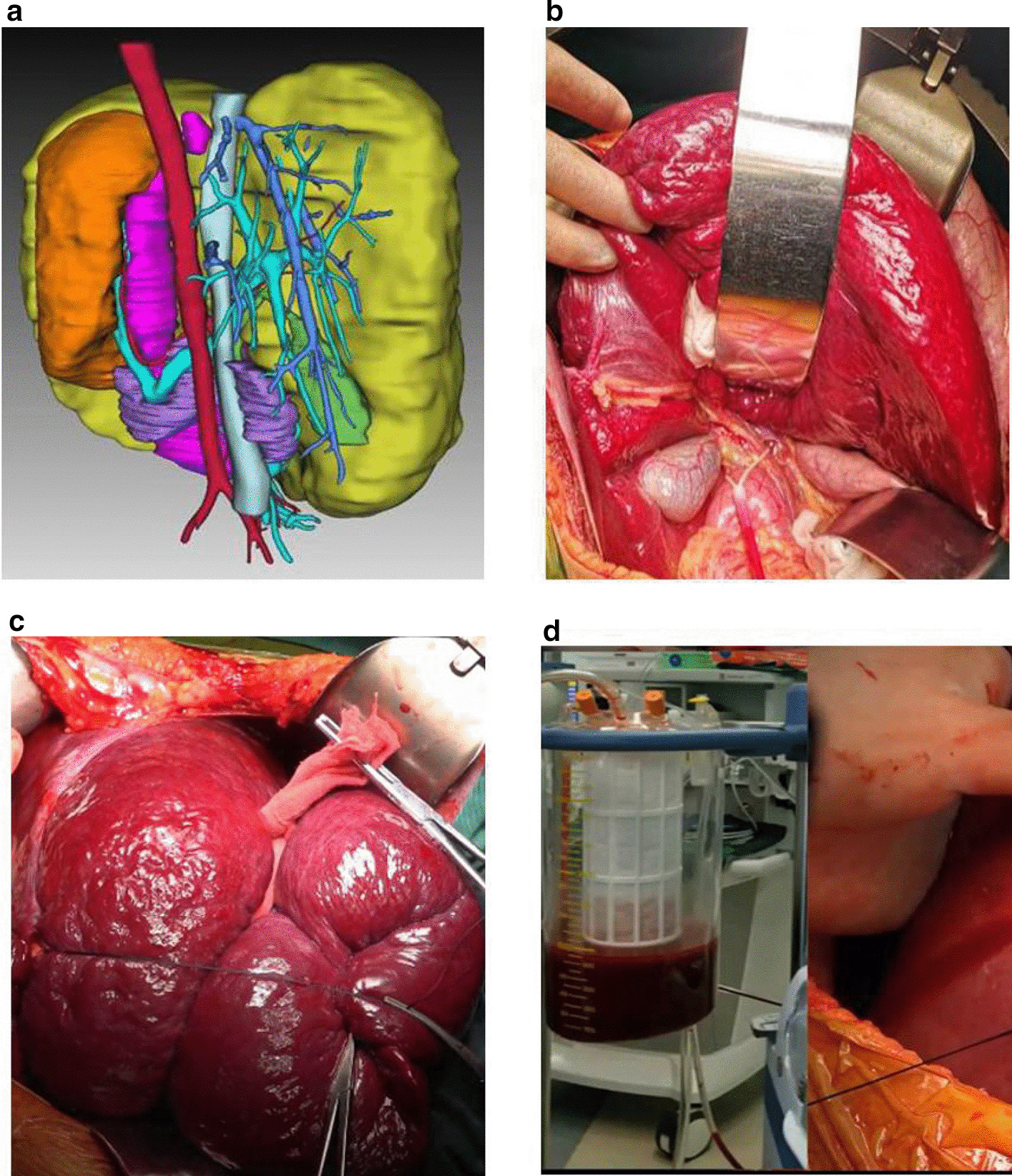
Methods: Data from 152 patients with hepatic hemangioma who underwent hepatectomy between 2004 and 2019 were retrospectively reviewed. We analyzed characteristics including tumor size, surgical parameters, and variables associated with Kasabach-Merritt syndrome and compared the outcomes of laparoscopic and open hepatectomy. Here, we describe surgical techniques for giant hepatic hemangioma and report on two meaningful cases.
Results: Most (63.8%) patients with hepatic hemangioma were asymptomatic. Most (86.4%) tumors from patients with Kasabach-Merritt syndrome were larger than 15 cm. Enucleation (30.9%), sectionectomy (28.9%), hemihepatectomy (25.7%), and the removal of more than half of the liver (14.5%) were performed through open (87.5%) and laparoscopic (12.5%) approaches. Laparoscopic hepatectomy is associated with an operative time, estimated blood loss, and major morbidity and mortality rate similar to those of open hepatectomy, but a shorter length of stay. 3D image reconstruction is an alternative for diagnosis and surgical planning for partial hepatectomy.
Conclusion: The main indication for surgery is giant (> 10 cm) liver hemangioma, with or without symptoms. Laparoscopic hepatectomy was an effective option for hepatic hemangioma treatment. For extremely giant hemangiomas, 3D image reconstruction was indispensable. Hepatectomy should be performed by experienced hepatic surgeons.
Keywords: 3D image reconstruction; Giant; Hepatic hemangioma; Surgical indication; Surgical management; Surgical technique.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
