

Protocadherin 7-Associated Membranous Nephropathy
- PMID: 33833079
- PMCID: PMC8259689
- DOI: 10.1681/ASN.2020081165
Protocadherin 7-Associated Membranous Nephropathy
Abstract
Background: Membranous nephropathy (MN) results from deposition of antigen-antibody complexes along the glomerular basement membrane (GBM). PLA2R, THSD7A, NELL1, and SEMA3B account for 80%-90% of target antigens in MN.
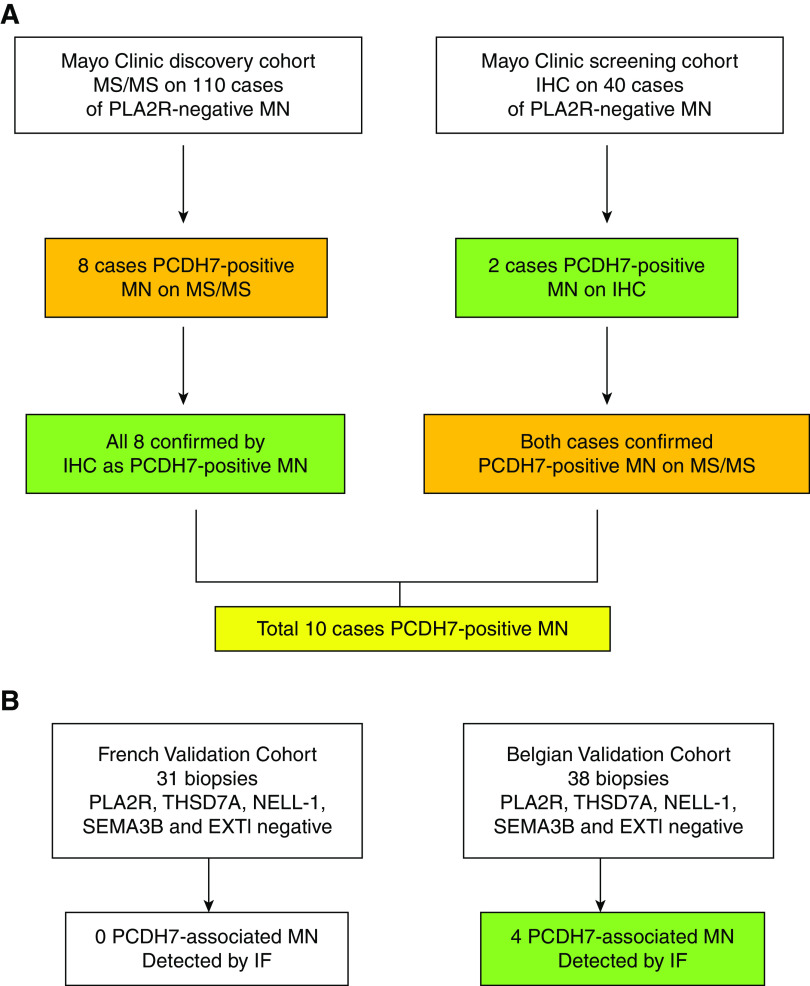
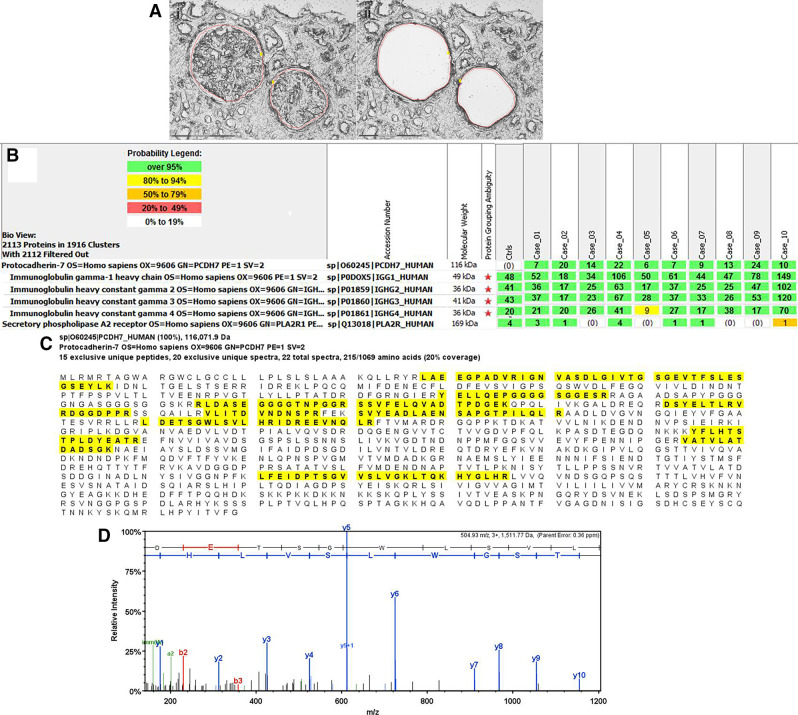
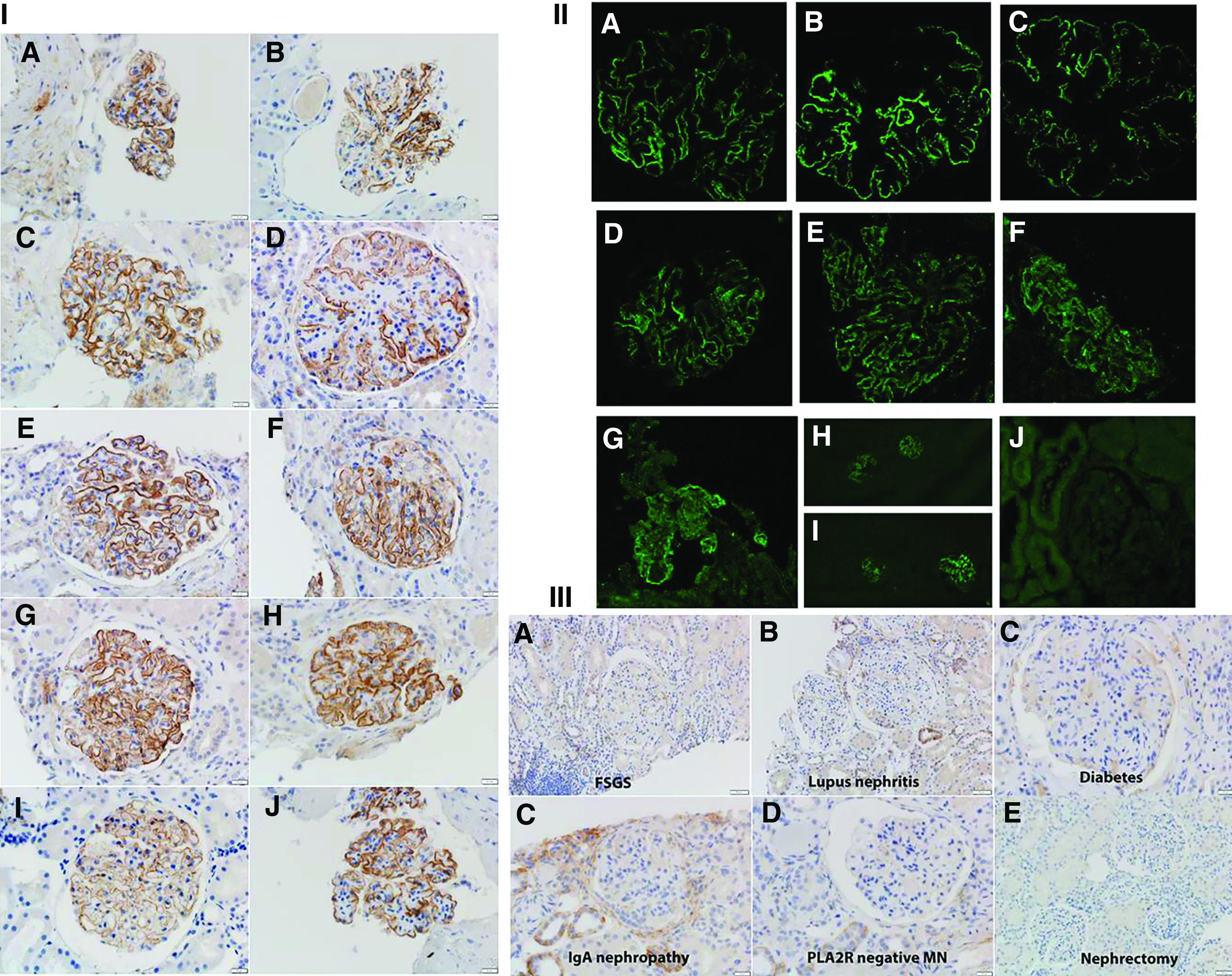
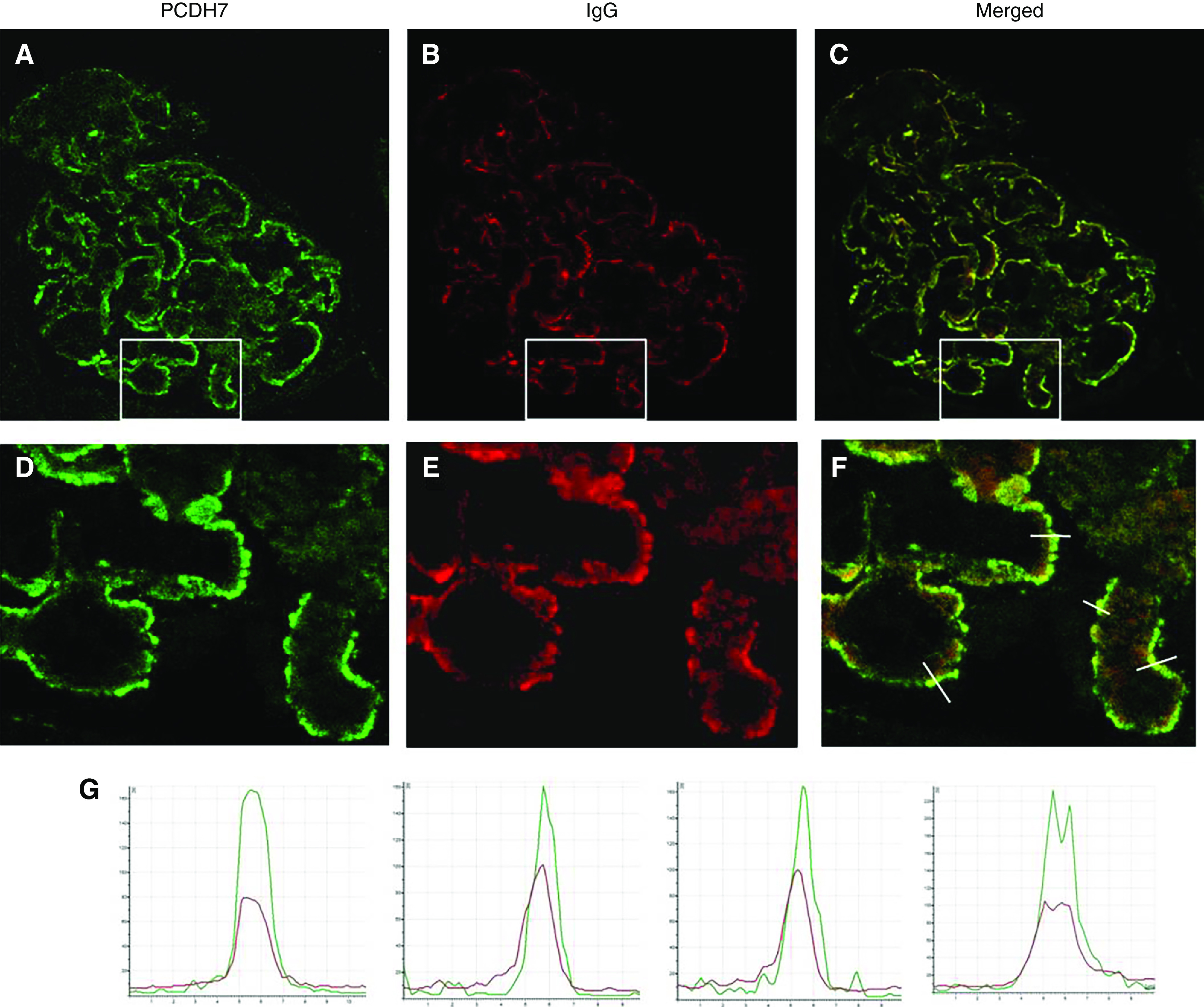
Methods: We performed laser microdissection and mass spectrometry (MS/MS) in kidney biopsies from 135 individuals with PLA2R-negative MN, and used immunohistochemistry/immunofluorescence and confocal microscopy to confirm the MS/MS finding, detect additional cases, and localize the novel protein. We also performed MS/MS and immunohistochemistry on 116 controls and used immunofluorescence microscopy to screen biopsy samples from two validation cohorts. Western blot and elution studies were performed to detect antibodies in serum and biopsy tissue.
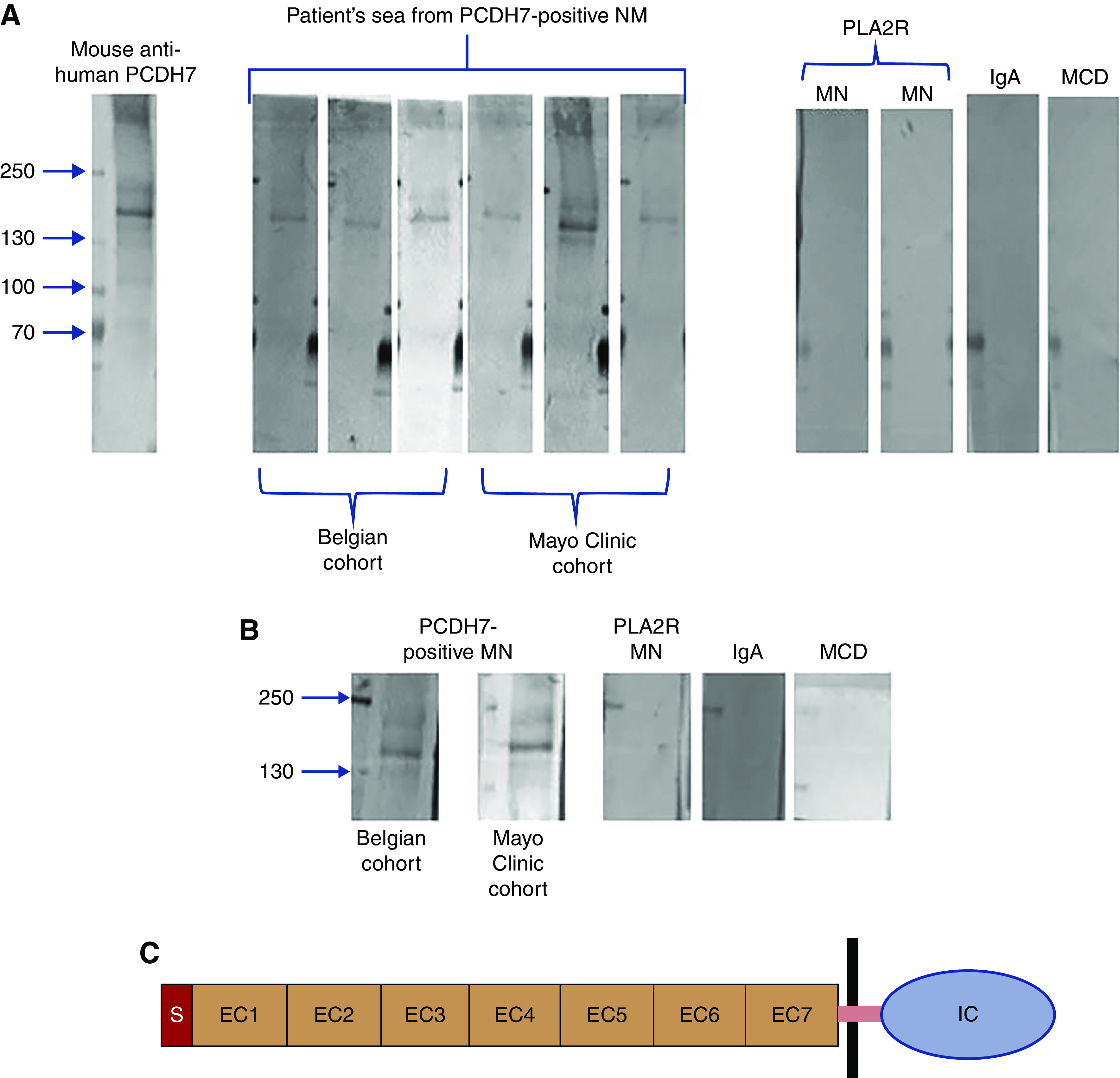
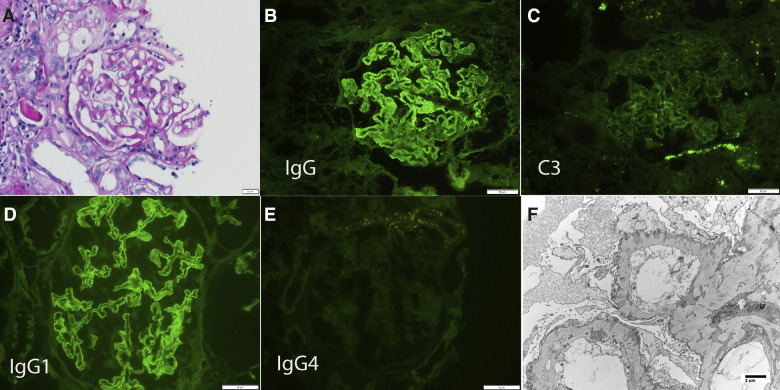
Results: MS/MS studies detected a unique protein, protocadherin 7 (PCDH7), in glomeruli of ten (5.7%) PLA2R-negative MN cases, which also were negative for PLA2R, THSD7A, EXT1/EXT2, NELL1, and SEMA3B. Spectral counts ranged from six to 24 (average 13.2 [SD 6.6]). MS/MS did not detect PCDH7 in controls (which included 28 PLA2R-positive cases). In all ten PCDH7-positive cases, immunohistochemistry showed bright granular staining along the GBM, which was absent in the remaining cases of PLA2R-negative MN and control cases. Four of 69 (5.8%) cases in the validation cohorts (all of which were negative for PLA2R, THSD7A, EXT1, NELL1, and SEMA3B) were PCDH7-positive MN. Kidney biopsy showed minimal complement deposition in 12 of the 14 PCDH7-associated cases. Confocal microscopy showed colocalization of PCDH7 and IgG along the GBM. Western blot analysis using sera from six patients showed antibodies to nonreduced PCDH7. Elution of IgG from frozen tissue of PCDH7-associated MN showed reactivity against PCDH7.
Conclusions: MN associated with the protocadherin PCDH7 appears to be a distinct, previously unidentified type of MN.
Keywords: glomerular disease; immunology and pathology; membranous nephropathy; nephrotic syndrome; renal biopsy; renal pathology.
Copyright © 2021 by the American Society of Nephrology.
Figures
References
-
- Ronco P, Debiec H: Pathophysiological advances in membranous nephropathy: Time for a shift in patient’s care. Lancet 385: 1983–1992, 2015. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
