

The role of chest CT quantitative pulmonary inflammatory index in the evaluation of the course and treatment outcome of COVID-19 pneumonia
- PMID: 33833340
- PMCID: PMC8032697
- DOI: 10.1038/s41598-021-87430-5
The role of chest CT quantitative pulmonary inflammatory index in the evaluation of the course and treatment outcome of COVID-19 pneumonia
Abstract
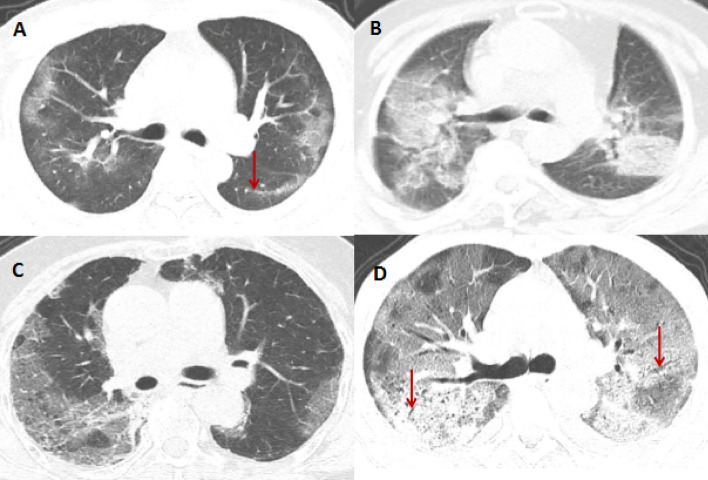
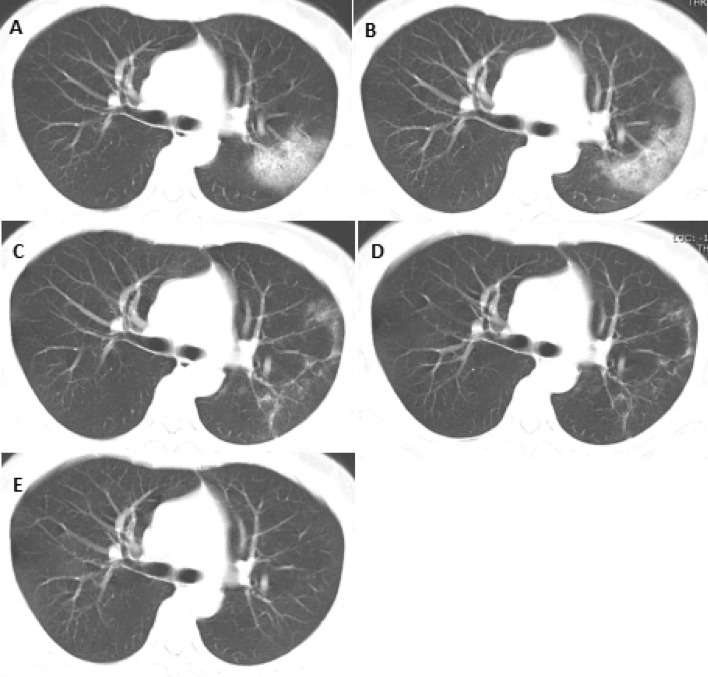
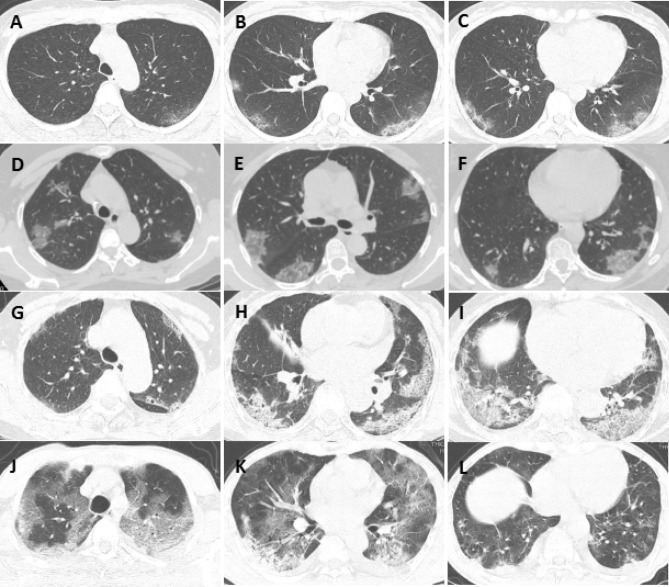
To explore the clinical application value of chest CT quantitative pulmonary inflammation index (PII) in the evaluation of the course and treatment outcome of COVID-19 pneumonia. One hundred and eighteen patients with COVID-19 pneumonia diagnosed by RT-PCR were analyzed retrospectively. The correlation between chest CT PII, clinical symptoms and laboratory examinations during the entire hospitalization period was compared. The average age of the patients was 46.0 ± 15 (range: 1-74) years. Of the 118 patients, 62 are male (52.5%) and 56 are female (47.5%). Among them, 116 patients recovered and were discharged, 2 patients died, and the median length of hospital stay was 22 (range: 9-41) days. On admission, 76.3% of the patients presented with fever, and the laboratory studies showed a decrease in lymphocyte (LYM) count and an increase in lactate dehydrogenase (LDH) levels, C-reactive protein (CRP) levels, and erythrocyte sedimentation rate (ESR). Within the studies' chest CTs, the median number of involved lung lobes was 4 (range: 0-5) and the median number of involved lung segments was 9 (range 0-20). The left lower lobe and the right lower lobe were the most likely areas to be involved (89.0% and 83.9%), and 84.7% of the patients had inflammatory changes in both lungs. The main manifestations on chest CT were ground glass opacities (31.4%), ground glass opacities and consolidation (20.3%), ground glass opacities and reticular patterns (32.2%), mixed type (13.6%), and white lungs (1.7%); common accompanying signs included linear opacities (55.9%), air bronchograms (46.6%), thick small vessel shadows (36.4%), and pleural hypertrophy (13.6%). The chest CT at discharge showed complete absorption of lesions in 19 cases (16.1%), but not in the remaining 99 cases. Lesions remained in a median of 3 lung lobes (range: 0-5). Residual lesions remained in a median of 5 lung segments (range: 0-20). The residual lesions mainly presented as ground glass opacities (61.0%), and the main accompanying sign was linear opacities (59.3%). Based on chest CT, the median maximum PII of lungs was 30.0% (range: 0-97.5%), and the median PII after discharge in the patients excluding the two deaths was 12.5% (range: 0-53.0%). PII was significantly negatively correlated with the LYM count and significantly positively correlated with body temperature, LDH, CRP, and ESR. There was no significant correlation between the PII and the white blood cell count, but the grade of PII correlated well with the clinical classification. PII can be used to monitor the severity and the treatment outcome of COVID-19 pneumonia, provide help for clinical classification, assist in treatment plan adjustments and aid assessments for discharge.
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
A new imaging sign in COVID-19 pneumonia: vascular changes and their correlation with clinical severity of the disease.Diagn Interv Radiol. 2021 Mar;27(2):172-180. doi: 10.5152/dir.2020.20346. Diagn Interv Radiol. 2021. PMID: 33044171 Free PMC article.
-
Preliminary CT findings of coronavirus disease 2019 (COVID-19).Clin Imaging. 2020 Sep;65:124-132. doi: 10.1016/j.clinimag.2020.04.042. Epub 2020 May 12. Clin Imaging. 2020. PMID: 32464579 Free PMC article.
-
Analysis of clinical features and imaging signs of COVID-19 with the assistance of artificial intelligence.Eur Rev Med Pharmacol Sci. 2020 Aug;24(15):8210-8218. doi: 10.26355/eurrev_202008_22510. Eur Rev Med Pharmacol Sci. 2020. PMID: 32767351
-
Computed tomography features of COVID-19 in children: A systematic review and meta-analysis.Medicine (Baltimore). 2021 Sep 24;100(38):e22571. doi: 10.1097/MD.0000000000022571. Medicine (Baltimore). 2021. PMID: 34559092 Free PMC article.
-
The novel coronavirus pneumonia (COVID-19): a pictorial review of chest CT features.Diagn Interv Radiol. 2021 Mar;27(2):188-194. doi: 10.5152/dir.2020.20304. Diagn Interv Radiol. 2021. PMID: 32815523 Free PMC article. Review.
Cited by
-
Association of Low Molecular Weight Plasma Aminothiols with the Severity of Coronavirus Disease 2019.Oxid Med Cell Longev. 2021 Sep 18;2021:9221693. doi: 10.1155/2021/9221693. eCollection 2021. Oxid Med Cell Longev. 2021. PMID: 34557267 Free PMC article.
-
Plasma S-Adenosylmethionine Is Associated with Lung Injury in COVID-19.Dis Markers. 2021 Dec 16;2021:7686374. doi: 10.1155/2021/7686374. eCollection 2021. Dis Markers. 2021. PMID: 34956420 Free PMC article.
-
3D Bioprinting for Regenerating COVID-19-Mediated Irreversibly Damaged Lung Tissue.Int J Bioprint. 2022 Sep 13;8(4):616. doi: 10.18063/ijb.v8i4.616. eCollection 2022. Int J Bioprint. 2022. PMID: 36404781 Free PMC article. Review.
-
Clinical efficacy of budesonide combined with acetylcysteine in the treatment of mycoplasma pneumonia infection.Immun Inflamm Dis. 2023 Nov;11(11):e1068. doi: 10.1002/iid3.1068. Immun Inflamm Dis. 2023. PMID: 38018572 Free PMC article.
-
Bacterial co-infection raises in-hospital mortality of COVID-19 patients: a retrospective study.Front Microbiol. 2023 Jun 29;14:1206476. doi: 10.3389/fmicb.2023.1206476. eCollection 2023. Front Microbiol. 2023. PMID: 37455733 Free PMC article.
References
-
- International Committee on Taxonomy of Virus. Naming the 2019 Coronavirus (2020) https://talk.ictvonline.org/. Accessed 2 Mar 2020.
-
- World Health Organization. WHO Director -General's remarks at the media briefing on 2019-nCoV on 11 February. 2020. (2020–02–11) [2020–02–20]. https://www.who.int/dg/speeches/detail/who-director-general-s-opening-re....
-
- General Office of National Health Committee. Office of State Administration of Traditional Chinese Medicine. Notice on the issuance of a program for the diagnosis and treatment of novel coronavirus (2019-nCoV) infected pneumonia (trial seventh edition) (2020–03–03).http://www.nhc.gov.cn/yzygj/s7653p/202003/46c9294a7dfe4cef80dc7f5912eb19....
-
- Chinese Society of Radiology. Radiological diagnosis of new coronavirus infected pneumonitis: Expert recommendation from the Chinese Society of Radiology (First edition). Chinese J. Radiol. 2020; Doi:10.3760/cma.j.issn.1005-1201.2020.0001.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
