

Clinical spectrum of MTOR-related hypomelanosis of Ito with neurodevelopmental abnormalities
- PMID: 33833411
- PMCID: PMC8354853
- DOI: 10.1038/s41436-021-01161-6
Clinical spectrum of MTOR-related hypomelanosis of Ito with neurodevelopmental abnormalities
Erratum in
-
Correction to: Clinical spectrum of MTOR-related hypomelanosis of Ito with neurodevelopmental abnormalities.Genet Med. 2021 Aug;23(8):1585. doi: 10.1038/s41436-021-01217-7. Genet Med. 2021. PMID: 34257424 Free PMC article. No abstract available.
Abstract
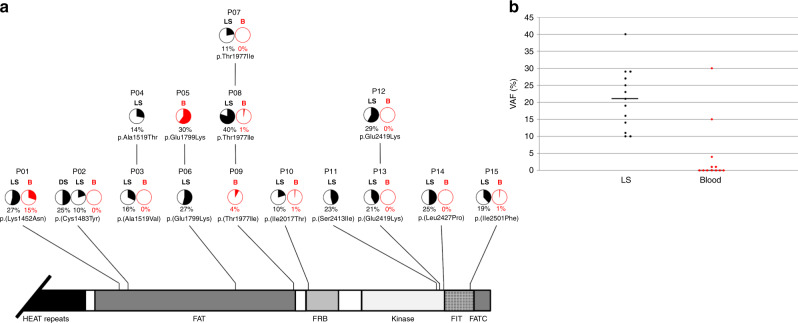
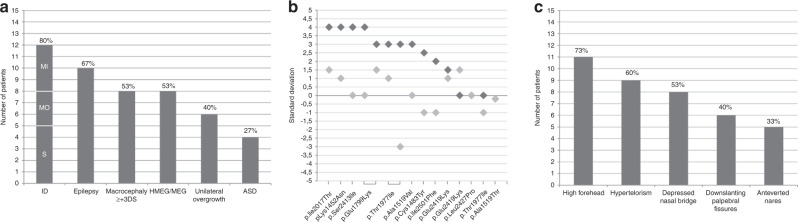
Purpose: Hypomelanosis of Ito (HI) is a skin marker of somatic mosaicism. Mosaic MTOR pathogenic variants have been reported in HI with brain overgrowth. We sought to delineate further the pigmentary skin phenotype and clinical spectrum of neurodevelopmental manifestations of MTOR-related HI.
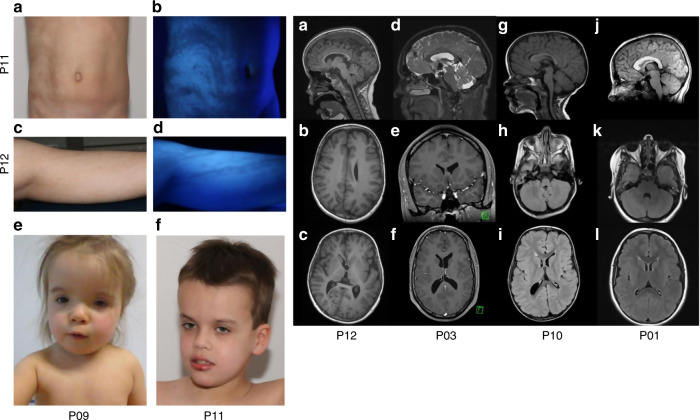
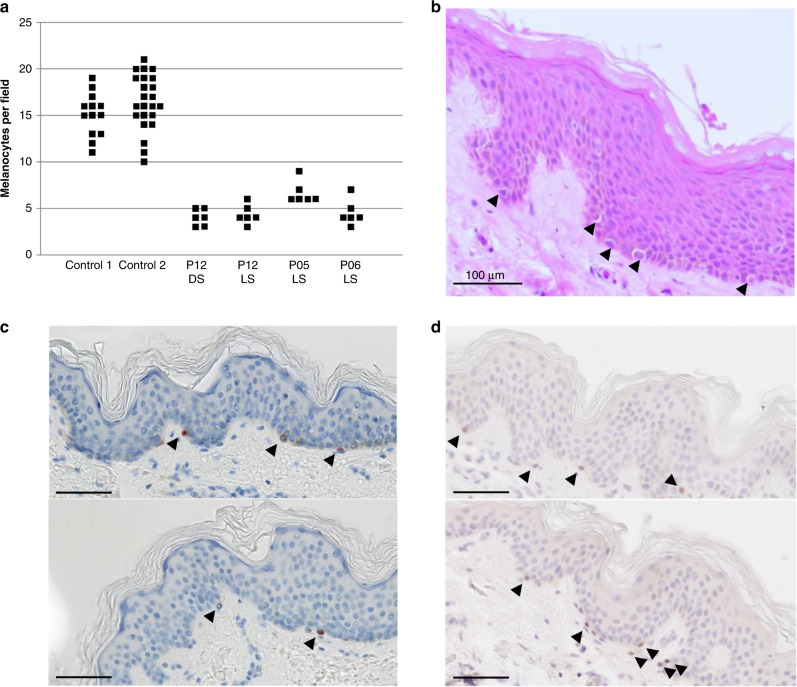
Methods: From two cohorts totaling 71 patients with pigmentary mosaicism, we identified 14 patients with Blaschko-linear and one with flag-like pigmentation abnormalities, psychomotor impairment or seizures, and a postzygotic MTOR variant in skin. Patient records, including brain magnetic resonance image (MRI) were reviewed. Immunostaining (n = 3) for melanocyte markers and ultrastructural studies (n = 2) were performed on skin biopsies.
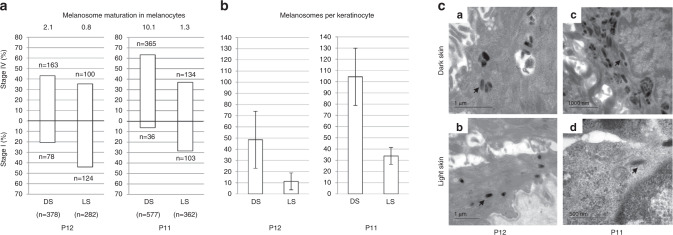
Results: MTOR variants were present in skin, but absent from blood in half of cases. In a patient (p.[Glu2419Lys] variant), phosphorylation of p70S6K was constitutively increased. In hypopigmented skin of two patients, we found a decrease in stage 4 melanosomes in melanocytes and keratinocytes. Most patients (80%) had macrocephaly or (hemi)megalencephaly on MRI.
Conclusion: MTOR-related HI is a recognizable neurocutaneous phenotype of patterned dyspigmentation, epilepsy, intellectual deficiency, and brain overgrowth, and a distinct subtype of hypomelanosis related to somatic mosaicism. Hypopigmentation may be due to a defect in melanogenesis, through mTORC1 activation, similar to hypochromic patches in tuberous sclerosis complex.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Response to Resta et al.Genet Med. 2021 Nov;23(11):2225. doi: 10.1038/s41436-021-01257-z. Epub 2021 Jul 7. Genet Med. 2021. PMID: 34234301 No abstract available.
-
Correspondence on "Clinical spectrum of MTOR-related hypomelanosis of Ito with neurodevelopmental abnormalities," by Carmignac et al.Genet Med. 2021 Nov;23(11):2223-2224. doi: 10.1038/s41436-021-01256-0. Epub 2021 Jul 7. Genet Med. 2021. PMID: 34234302 No abstract available.
References
-
- >Ito M. Incontinentia pigmenti achromians. A singular case of nevus depigmentosus systematicus bilateralis. Tohoku J. Exp. Med. 1952;55:57–59.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
