

SARS-CoV-2 and Human Immunodeficiency Virus: Pathogen Pincer Attack
- PMID: 33833585
- PMCID: PMC8020331
- DOI: 10.2147/HIV.S300055
SARS-CoV-2 and Human Immunodeficiency Virus: Pathogen Pincer Attack
Abstract
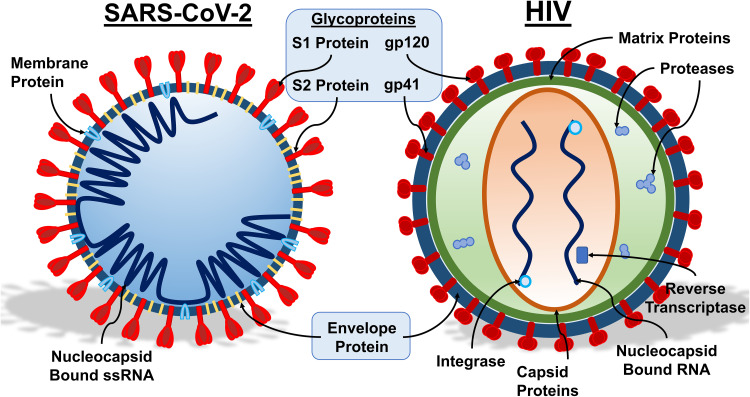
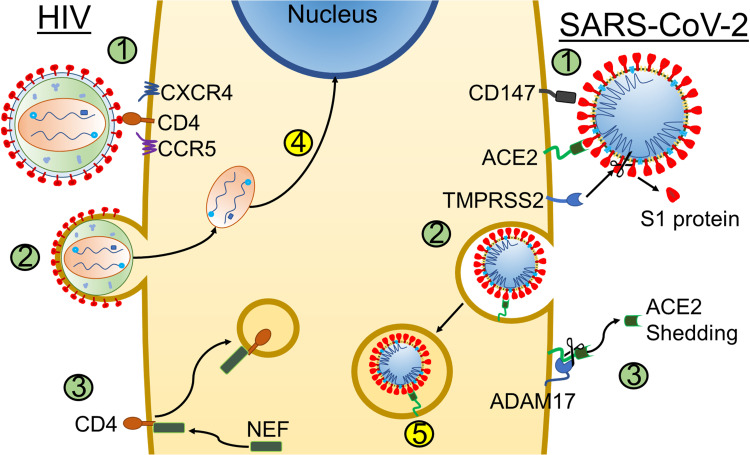
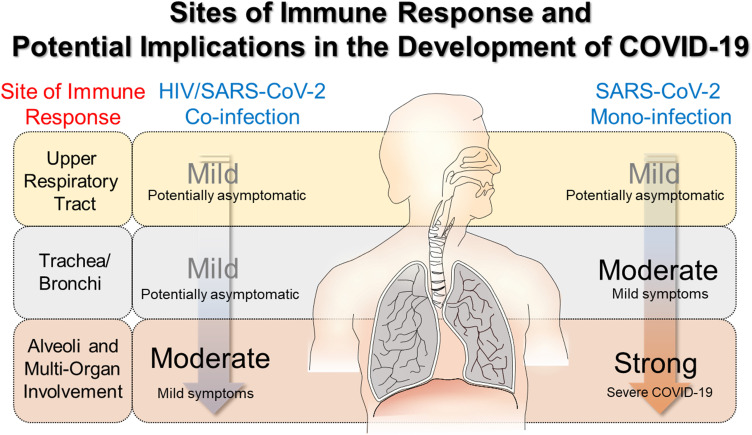
Paramount efforts worldwide are seeking to increase understanding of the basic virology of SARS-CoV-2, characterize the spectrum of complications associated with COVID-19, and develop vaccines that can protect from new and recurrent infections with SARS-CoV-2. While we continue learning about this new virus, it is clear that 1) the virus is spread via the respiratory route, primarily by droplets and contact with contaminated surfaces and fomites, as well as by aerosol formation during invasive respiratory procedures; 2) the airborne route is still controversial; and 3) that those infected can spread the virus without necessarily developing COVID-19 (ie, asymptomatic). With the number of SARS-CoV-2 infections increasing globally, the possibility of co-infections and/or co-morbidities is becoming more concerning. Co-infection with Human Immunodeficiency Virus (HIV) is one such example of polyparasitism of interest. This military-themed comparative review of SARS-CoV-2 and HIV details their virology and describes them figuratively as separate enemy armies. HIV, an old enemy dug into trenches in individuals already infected, and SARS-CoV-2 the new army, attempting to attack and capture territories, tissues and organs, in order to provide resources for their expansion. This analogy serves to aid in discussion of three main areas of focus and draw attention to how these viruses may cooperate to gain the upper hand in securing a host. Here we compare their target, the key receptors found on those tissues, viral lifecycles and tactics for immune response surveillance. The last focus is on the immune response to infection, addressing similarities in cytokines released. While the majority of HIV cases can be successfully managed with antiretroviral therapy nowadays, treatments for SARS-CoV-2 are still undergoing research given the novelty of this army.
Keywords: ACE-2; AIDS; COVID-19; HIV; SARS-CoV-2; remdesivir.
© 2021 Evans et al.
Conflict of interest statement
Dr Nicola Petrosillo report personal fees from Pfizer, Speakers’ bureau from MSD, Shionogi, Becton & Dickinson, Johnson & Johnson, Cepheid, outside the submitted work. The authors report no other conflicts of interest in this work.
Figures
Similar articles
-
Comparative Analysis of Virology and Pathogenesis of SARS-CoV-2 and HIV Infections: Implications for Public Health and Treatment Strategies.Infect Drug Resist. 2025 Jan 15;18:269-283. doi: 10.2147/IDR.S498430. eCollection 2025. Infect Drug Resist. 2025. PMID: 39835166 Free PMC article. Review.
-
Infection Prevention Precautions for Routine Anesthesia Care During the SARS-CoV-2 Pandemic.Anesth Analg. 2020 Nov;131(5):1342-1354. doi: 10.1213/ANE.0000000000005169. Anesth Analg. 2020. PMID: 33079853 Review.
-
A new pharmacological approach based on remdesivir aerosolized administration on SARS-CoV-2 pulmonary inflammation: A possible and rational therapeutic application.Med Hypotheses. 2020 Nov;144:109876. doi: 10.1016/j.mehy.2020.109876. Epub 2020 May 24. Med Hypotheses. 2020. PMID: 32562915 Free PMC article.
-
Deposition distribution of the new coronavirus (SARS-CoV-2) in the human airways upon exposure to cough-generated droplets and aerosol particles.Sci Rep. 2020 Dec 31;10(1):22430. doi: 10.1038/s41598-020-79985-6. Sci Rep. 2020. PMID: 33384436 Free PMC article.
-
Airborne transmission of SARS-CoV-2 is the dominant route of transmission: droplets and aerosols.Infez Med. 2021 Mar 1;29(1):10-19. Infez Med. 2021. PMID: 33664169 Review.
Cited by
-
A computational overview of integrase strand transfer inhibitors (INSTIs) against emerging and evolving drug-resistant HIV-1 integrase mutants.Arch Microbiol. 2023 Mar 26;205(4):142. doi: 10.1007/s00203-023-03461-8. Arch Microbiol. 2023. PMID: 36966200 Free PMC article. Review.
-
Stability analysis of within-host SARS-CoV-2/HIV coinfection model.Math Methods Appl Sci. 2022 Jun 3:10.1002/mma.8457. doi: 10.1002/mma.8457. Online ahead of print. Math Methods Appl Sci. 2022. PMID: 35942149 Free PMC article.
-
The Impact of COVID-19 on People Living with HIV-1 and HIV-1-Associated Neurological Complications.Viruses. 2023 May 5;15(5):1117. doi: 10.3390/v15051117. Viruses. 2023. PMID: 37243203 Free PMC article. Review.
-
COVID-19 in HIV-positive patients: A systematic review of case reports and case series.J Clin Lab Anal. 2022 Apr;36(4):e24308. doi: 10.1002/jcla.24308. Epub 2022 Feb 20. J Clin Lab Anal. 2022. PMID: 35187723 Free PMC article.
-
Global analysis of within-host SARS-CoV-2/HIV coinfection model with latency.Eur Phys J Plus. 2022;137(2):174. doi: 10.1140/epjp/s13360-022-02387-2. Epub 2022 Jan 27. Eur Phys J Plus. 2022. PMID: 35106266 Free PMC article.
References
-
- Gottlieb MS, Fan PT, Saxon A, Weisman JD. Pneumocystis Pneumonia—Los Angeles. Morbidity and Mortality Weekly Rep. 1981;30(21):1–3. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
