

Factors Associated with Low Uptake of Voluntary Medical Male Circumcision as HIV-Prevention Strategy among Men Aged 18-49 Years from Nyanza District, Rwanda
- PMID: 33833586
- PMCID: PMC8021263
- DOI: 10.2147/HIV.S301045
Factors Associated with Low Uptake of Voluntary Medical Male Circumcision as HIV-Prevention Strategy among Men Aged 18-49 Years from Nyanza District, Rwanda
Abstract
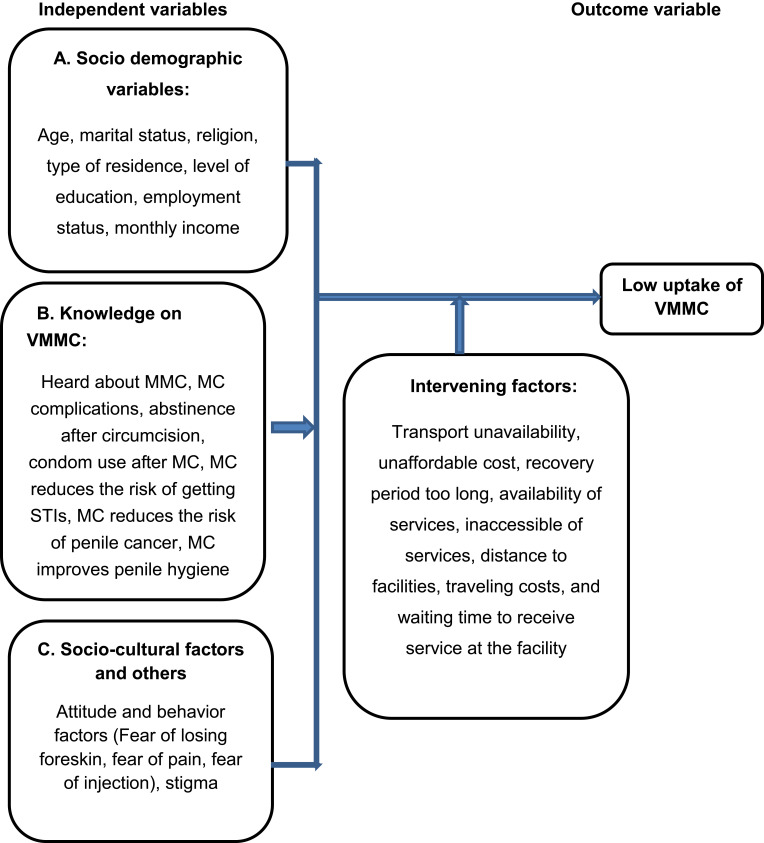
Background: Voluntary medical male circumcision (VMMC) is an effective biomedical intervention against HIV in developed and developing countries. However, there is low uptake of VMMC due to various factors, which hinders achievement of health-policy goals to increase uptake. Numerous campaigns offering the procedure free of charge exist in developing countries, but such initiatives seem to bear little fruit in attracting men to these services. This study assessed risk factors associated with the low uptake of VMMC among men in Nyanza district, Southern Province, Rwanda.
Methods: A cross-sectional study was conducted among adult males in Nyanza. A total of 438 men participated in individual interviews. Bivariate and multivariate logistic regression models were used with 95% confidence intervals and p≤0.05 was taken as statistically significant.
Results: Our results indicated that a low update of VMMC was highly prevalent (35.8%). A majority (84.7%) of participants had heard about VMMC, its complications, advantages in preventiing penile cancer, sexually transmitted infections, and HIV, condom use after circumcision, abstinence for 6 weeks after circumcision, and improving penile hygiene. Religion and education were significant factors in low uptake. Catholics were less likely to undergo VMMC than Muslims (OR 7.19, 95% CI 1.742-29.659; p=0.01). Those of other faiths were less likely to undergo VMMC than Muslims (OR 6.035, 95% CI 1.731-21.039; p=0.005). Participants with secondary education were less likely to undergo VMMC than those with primary education only (OR 1.4, 95% CI 0.74-2.64; p=0.03). Having no formal education decreased the odds of being uncircumcised (OR 0.37, 95% CI 0.14-0.977; p=0.045) when compared to those with primary education.
Conclusion: Uptake of VMMC remains low in Nyanza, but most men had sufficient knowledge about it. Education, religion, and marital status were major factors in the low uptake. Programs targeting peer influences and parents need to be prioritized.
Keywords: HIV/AIDS; VMMC; adult; low uptake; male circumcision; men; prevention.
© 2021 Nzamwita and Biracyaza.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Evidence that promotion of male circumcision did not lead to sexual risk compensation in prioritized Sub-Saharan countries.PLoS One. 2017 Apr 25;12(4):e0175928. doi: 10.1371/journal.pone.0175928. eCollection 2017. PLoS One. 2017. PMID: 28441458 Free PMC article.
-
FACTORS INFLUENCING VOLUNTARY MEDICAL MALE CIRCUMCISION AMONG MEN AGED 18-50 YEARS IN KIBERA DIVISION.East Afr Med J. 2014 Nov;91(11):407-13. East Afr Med J. 2014. PMID: 26866089
-
Missed opportunity: low uptake of VMMC among men attending the OPD of a public health facility offering free VMMC services in Uganda.BMC Public Health. 2023 Jan 18;23(1):129. doi: 10.1186/s12889-023-15056-5. BMC Public Health. 2023. PMID: 36653836 Free PMC article.
-
Voluntary medical male circumcision: an HIV prevention priority for PEPFAR.J Acquir Immune Defic Syndr. 2012 Aug 15;60 Suppl 3(0 3):S88-95. doi: 10.1097/QAI.0b013e31825cac4e. J Acquir Immune Defic Syndr. 2012. PMID: 22797745 Free PMC article. Review.
-
Voluntary medical male circumcision: translating research into the rapid expansion of services in Kenya, 2008-2011.PLoS Med. 2011 Nov;8(11):e1001130. doi: 10.1371/journal.pmed.1001130. Epub 2011 Nov 29. PLoS Med. 2011. PMID: 22140365 Free PMC article. Review.
Cited by
-
Knowledge and Attitudes of Circumcision among Adult Male Clients Receiving Care in a Teaching Hospital in Kigali City, Rwanda.Rwanda J Med Health Sci. 2024 Jul 31;7(2):359-371. doi: 10.4314/rjmhs.v7i2.21. eCollection 2024 Jul. Rwanda J Med Health Sci. 2024. PMID: 40567845 Free PMC article.
-
Factors Associated with Low Uptake of Medical Male Circumcision Among Adolescent Boys in Tanzania: A Multinomial Logistic Regression Modeling.HIV AIDS (Auckl). 2022 Dec 19;14:565-575. doi: 10.2147/HIV.S387380. eCollection 2022. HIV AIDS (Auckl). 2022. PMID: 36571074 Free PMC article.
-
Knowledge, Perception, and Practice of Safe Medical Circumcision on HIV Infection Risk Reduction among Undergraduate Students of a Public University in Northern Uganda: A Cross-Sectional Study.Biomed Res Int. 2024 Apr 9;2024:1534139. doi: 10.1155/2024/1534139. eCollection 2024. Biomed Res Int. 2024. PMID: 38633241 Free PMC article.
-
Estimates of the prevalence of male circumcision in sub-Saharan Africa from 2010-2023-A systematic review and meta-analysis.PLoS One. 2024 Mar 13;19(3):e0298387. doi: 10.1371/journal.pone.0298387. eCollection 2024. PLoS One. 2024. PMID: 38478528 Free PMC article.
-
Men undergoing medical circumcision at a community health centre: Knowledge and attitudes.S Afr Fam Pract (2004). 2025 Mar 21;67(1):e1-e7. doi: 10.4102/safp.v67i1.6010. S Afr Fam Pract (2004). 2025. PMID: 40171714 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
