

Association Between Early Administration of Norepinephrine in Septic Shock and Survival
- PMID: 33833595
- PMCID: PMC8020327
- DOI: 10.2147/OAEM.S298315
Association Between Early Administration of Norepinephrine in Septic Shock and Survival
Abstract
Introduction: Septic shock still carries a high mortality rate despite all advances in emergency and critical care practices. Early interventions have been proven in many aspects to improve outcome. However, early administration of vasopressors namely norepinephrine in septic shock is still controversial.
Objective: To identify the association between early norepinephrine administration and mortality in septic shock patients.
Methods: A retrospective review of a prospectively collected ICU data for septic shock patients in medical and surgical intensive care units for one year period was carried out. Case definition was based on sepsis 3 definitions. Data included patients' characteristics of demographics, admission diagnosis, APACHE II score, physiological data (including vital signs and laboratory values). The primary outcome was 28 days of mortality.
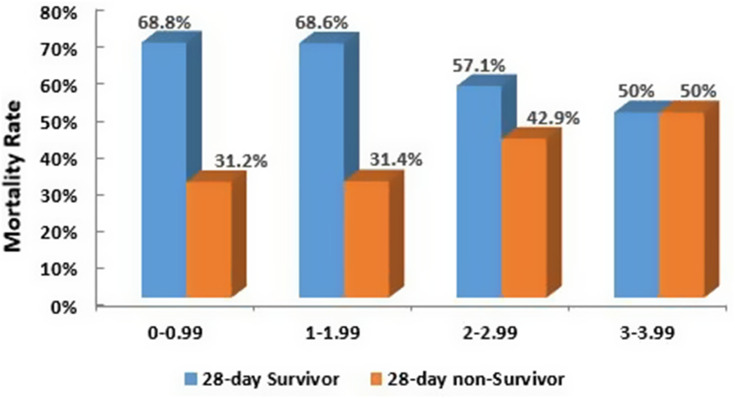
Results: A total of 243 patients identified during the study period, 132 (54.3%) were male. The mean age was found to be 58.9 ± 20.3. The overall rate of 28 days mortality was 87 (47.5%). Norepinephrine was started for 68.9% of the patients in ICU, the rest were started in the emergency department. The highest survival rates were among patients who received norepinephrine within first hour (58.1%) and second (51.5%). A binary logistic regression analysis has been performed to adjust for possible confounders. It was revealed that being intubated and mechanically ventilated or having higher APACHE II score were strongly associated with non-survival rates (OR=7.049, p-0.002), (OR=1.124, p-<0.001) respectively.
Conclusion: Our results showed that septic shock patients who had early administration of norepinephrine had a higher survival rate. Intubation and invasive ventilation and higher APACHE II score associated with higher none survival rate.
Keywords: antibacterial agents; sepsis; septic shock.
© 2021 Alshahrani and Alatigue.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Clinical management for patients admitted to a critical care unit with severe sepsis or septic shock.Intensive Crit Care Nurs. 2015 Dec;31(6):359-65. doi: 10.1016/j.iccn.2015.04.005. Epub 2015 Aug 17. Intensive Crit Care Nurs. 2015. PMID: 26292920
-
Sepsis Care Pathway 2019.Qatar Med J. 2019 Nov 7;2019(2):4. doi: 10.5339/qmj.2019.qccc.4. eCollection 2019. Qatar Med J. 2019. PMID: 31763206 Free PMC article.
-
[Study on the value of prothrombin time for predicting the severity and prognosis of septic patients].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2022 Jul;34(7):682-688. doi: 10.3760/cma.j.cn121430-20210614-00876. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2022. PMID: 36100403 Chinese.
-
Early lactate clearance is associated with improved outcome in severe sepsis and septic shock.Crit Care Med. 2004 Aug;32(8):1637-42. doi: 10.1097/01.ccm.0000132904.35713.a7. Crit Care Med. 2004. PMID: 15286537 Clinical Trial.
-
Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012.Crit Care Med. 2013 Feb;41(2):580-637. doi: 10.1097/CCM.0b013e31827e83af. Crit Care Med. 2013. PMID: 23353941
Cited by
-
Sex- and Gender-Based Analysis on Norepinephrine Use in Septic Shock: Why Is It Still a Male World?Microorganisms. 2024 Apr 18;12(4):821. doi: 10.3390/microorganisms12040821. Microorganisms. 2024. PMID: 38674765 Free PMC article.
-
2023 Update on Sepsis and Septic Shock in Adult Patients: Management in the Emergency Department.J Clin Med. 2023 Apr 28;12(9):3188. doi: 10.3390/jcm12093188. J Clin Med. 2023. PMID: 37176628 Free PMC article. Review.
-
Effect of timing of norepinephrine administration on prognosis of patients with septic shock: A prospective cohort study.J Intensive Med. 2024 Nov 29;5(2):160-166. doi: 10.1016/j.jointm.2024.10.002. eCollection 2025 Apr. J Intensive Med. 2024. PMID: 40241840 Free PMC article.
References
-
- Rowan K, Angus D, Bailey M, Barnato A. Early, goal-directed therapy for septic shock—a patient-level meta-analysis. N Engl J Med. 2017;376(23):2223–2234. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
