

Neurophysiologic Profiling of At-Risk Low and Very Low Birth-Weight Infants Using Magnetic Resonance Imaging
- PMID: 33833688
- PMCID: PMC8021729
- DOI: 10.3389/fphys.2021.638868
Neurophysiologic Profiling of At-Risk Low and Very Low Birth-Weight Infants Using Magnetic Resonance Imaging
Abstract
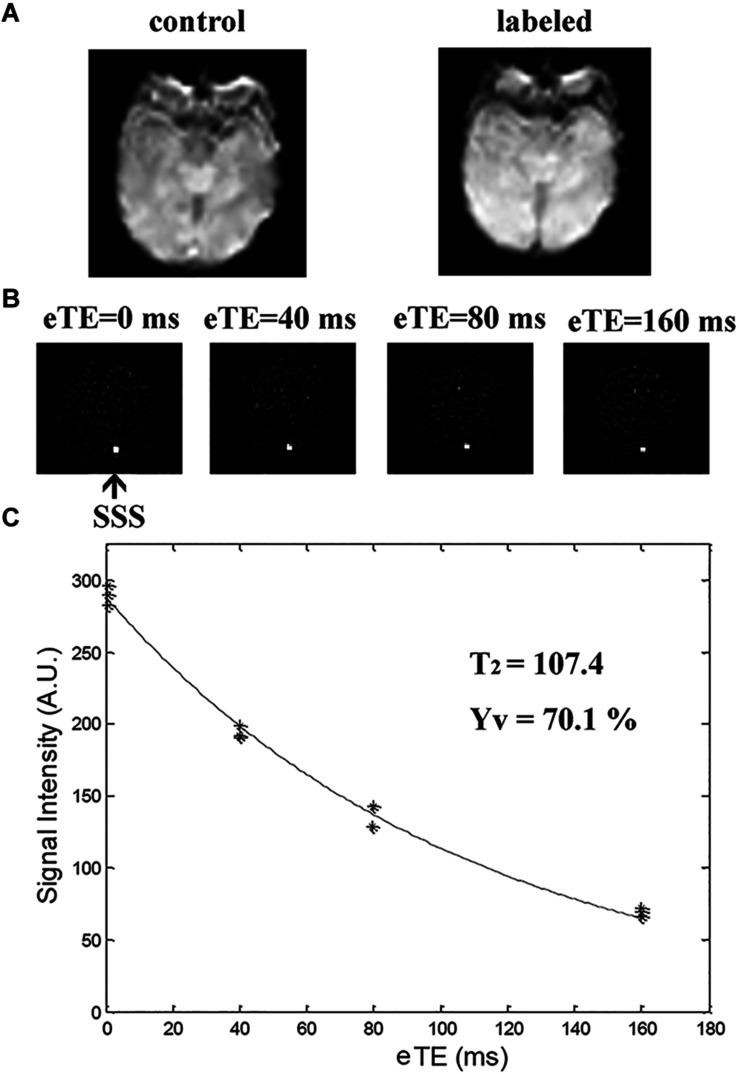
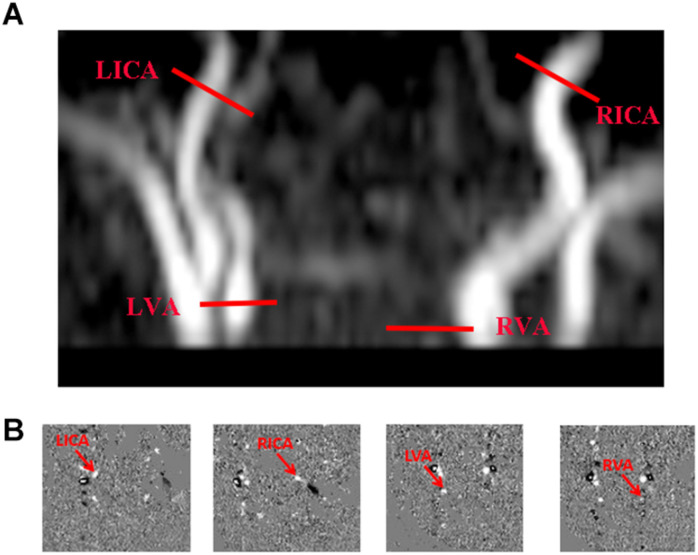
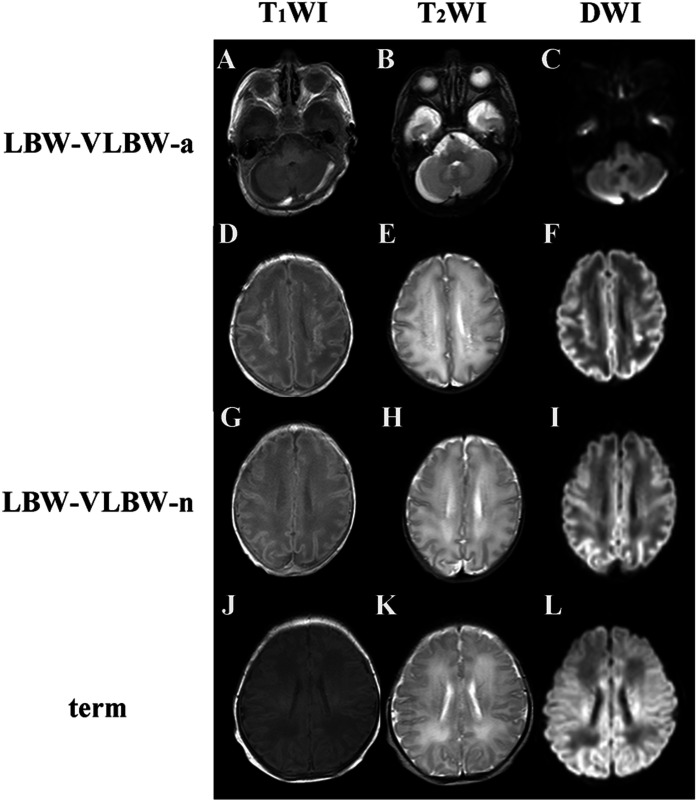
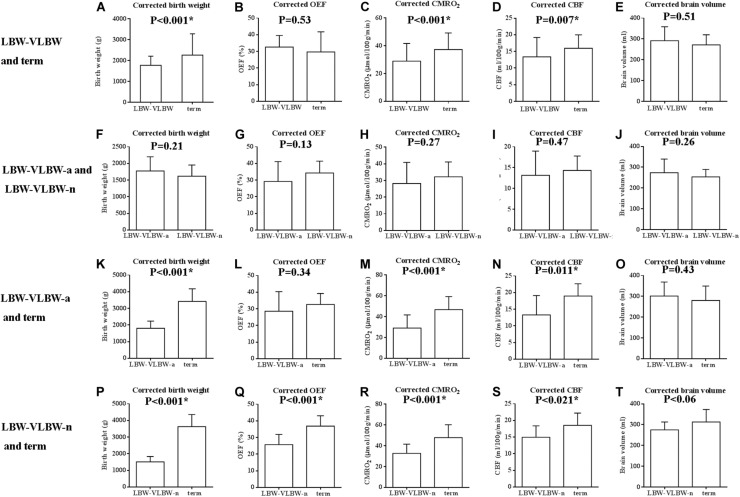
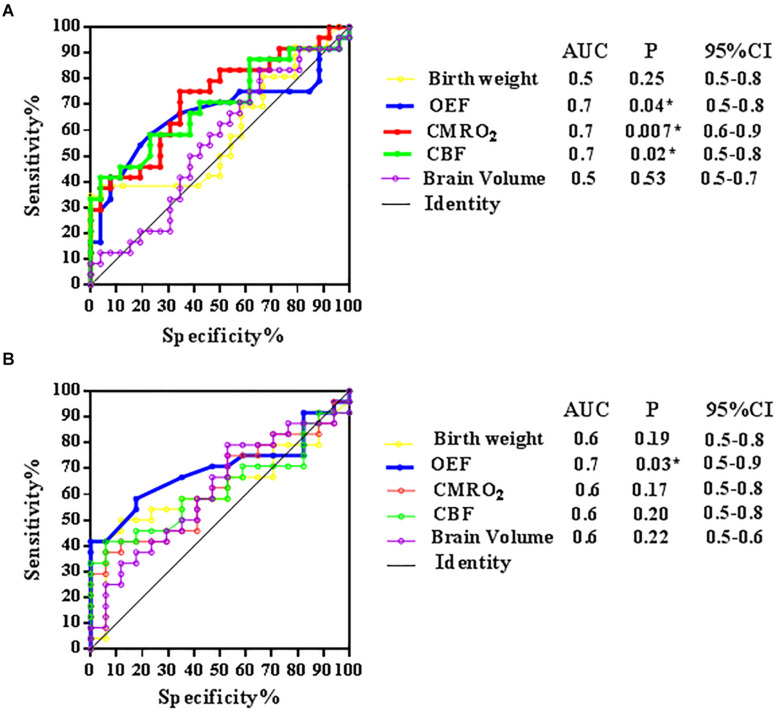
Low birth-weight (LBW) and very low birth-weight (VLBW) newborns have increased risks of brain injuries, growth failure, motor difficulties, developmental coordination disorders or delay, and adult-onset vascular diseases. However, relatively little is known of the neurobiologic underpinnings. To clarify the pathophysiologic vulnerabilities of such neonates, we applied several advanced techniques for assessing brain physiology, namely T2-relaxation-under-spin-tagging (TRUST) magnetic resonance imaging (MRI) and phase-contrast (PC) MRI. This enabled quantification of oxygen extraction fraction (OEF), global cerebral blood flow (CBF), and cerebral metabolic rate of oxygen (CMRO2). A total of 50 neonates (LBW-VLBW, 41; term controls, 9) participated in this study. LBW-VLBW neonates were further stratified as those with (LBW-VLBW-a, 24) and without (LBW-VLBW-n, 17) structural MRI (sMRI) abnormalities. TRUST and PC MRI studies were undertaken to determine OEF, CBF, and CMRO2. Ultimately, CMRO2 proved significantly lower (p = 0.01) in LBW-VLBW (vs term) neonates, both LBW-VLBW-a and LBW-VLBW-n subsets showing significantly greater physiologic deficits than term controls (p = 0.03 and p = 0.04, respectively). CMRO2 and CBF in LBW-VLBW-a and LBW-VLBW-n subsets did not differ significantly (p > 0.05), although OEF showed a tendency to diverge (p = 0.15). However, OEF values in the LBW-VLBW-n subset differed significantly from those of term controls (p = 0.02). Compared with brain volume or body weight, these physiologic parameters yield higher area-under-the-curve (AUC) values for distinguishing neonates of the LBW-VLBW-a subset. The latter displayed distinct cerebral metabolic and hemodynamic, whereas changes were marginal in the LBW-VLBW-n subset (i.e., higher OEF and lower CBF and CMRO2) by comparison. Physiologic imaging may therefore be useful in identifying LBW-VLBW newborns at high risk of irreversible brain damage.
Keywords: CBF; CMRO2; OEF; PC MRI; TRUST MRI; low birth weight (LBW); very low birth weight (VLBW).
Copyright © 2021 Qi and He.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Quantitative assessment of cerebral metabolism and hemodynamics in small-for-gestational-age (SGA) newborns.Quant Imaging Med Surg. 2021 Jun;11(6):2321-2332. doi: 10.21037/qims-20-1040. Quant Imaging Med Surg. 2021. PMID: 34079704 Free PMC article.
-
Hemodynamic and Metabolic Assessment of Neonates With Punctate White Matter Lesions Using Phase-Contrast MRI and T2-Relaxation-Under-Spin-Tagging (TRUST) MRI.Front Physiol. 2018 Mar 19;9:233. doi: 10.3389/fphys.2018.00233. eCollection 2018. Front Physiol. 2018. PMID: 29615927 Free PMC article.
-
Multi-Parametric Evaluation of Cerebral Hemodynamics in Neonatal Piglets Using Non-Contrast-Enhanced Magnetic Resonance Imaging Methods.J Magn Reson Imaging. 2021 Oct;54(4):1053-1065. doi: 10.1002/jmri.27638. Epub 2021 May 6. J Magn Reson Imaging. 2021. PMID: 33955613 Free PMC article.
-
Elevated global cerebral blood flow, oxygen extraction fraction and unchanged metabolic rate of oxygen in young adults with end-stage renal disease: an MRI study.Eur Radiol. 2016 Jun;26(6):1732-41. doi: 10.1007/s00330-015-3968-9. Epub 2015 Sep 3. Eur Radiol. 2016. PMID: 26334507
-
The Association Between Pregnancy-Induced Hypertension and Neonatal Cerebral Metabolism, Hemodynamics, and Brain Injury as Determined by Physiological Imaging.Front Physiol. 2022 Feb 28;13:756386. doi: 10.3389/fphys.2022.756386. eCollection 2022. Front Physiol. 2022. PMID: 35295587 Free PMC article.
Cited by
-
Measuring Quantitative Cerebral Blood Flow in Healthy Children: A Systematic Review of Neuroimaging Techniques.J Magn Reson Imaging. 2024 Jan;59(1):70-81. doi: 10.1002/jmri.28758. Epub 2023 May 11. J Magn Reson Imaging. 2024. PMID: 37170640 Free PMC article.
-
Cerebrovascular reactivity to carbon dioxide tension in newborns: data from combined time-resolved near-infrared spectroscopy and diffuse correlation spectroscopy.Neurophotonics. 2023 Oct;10(4):045003. doi: 10.1117/1.NPh.10.4.045003. Epub 2023 Oct 14. Neurophotonics. 2023. PMID: 37841558 Free PMC article.
-
Evaluation of the effects of prenatal exposure to pregabalin and postnatal analysis of dental and mandibular bone tissue development in rat offspring.Odontology. 2025 Mar 24. doi: 10.1007/s10266-025-01090-9. Online ahead of print. Odontology. 2025. PMID: 40126790
References
LinkOut - more resources
Full Text Sources
Other Literature Sources