

A New Neurorehabilitative Postsurgery Intervention for Facial Palsy Based on Smile Observation and Hand-Mouth Motor Synergies
- PMID: 33833792
- PMCID: PMC8016575
- DOI: 10.1155/2021/8890541
A New Neurorehabilitative Postsurgery Intervention for Facial Palsy Based on Smile Observation and Hand-Mouth Motor Synergies
Abstract
Objective: To perform a preliminary test of a new rehabilitation treatment (FIT-SAT), based on mirror mechanisms, for gracile muscles after smile surgery.
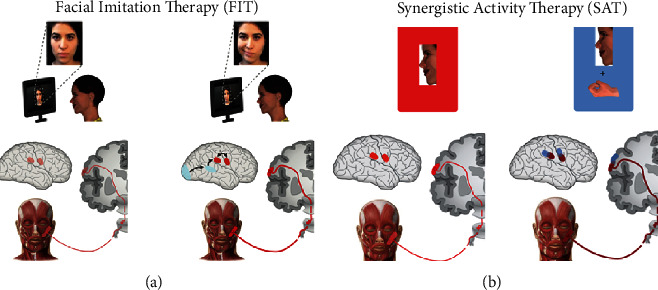
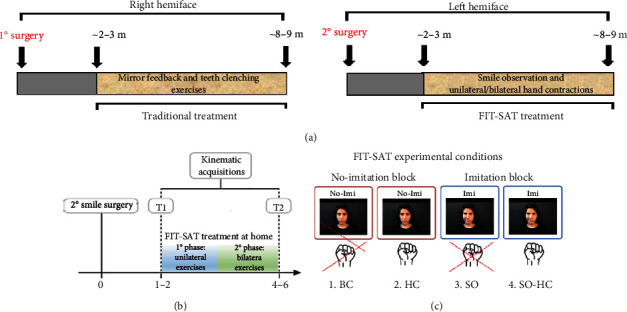
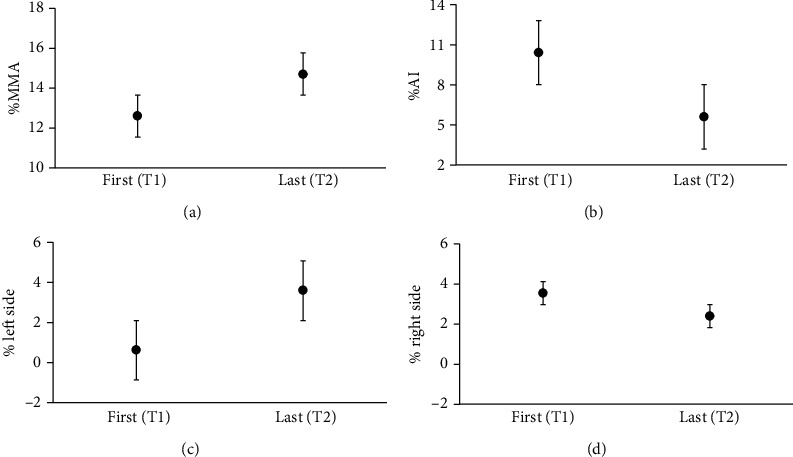
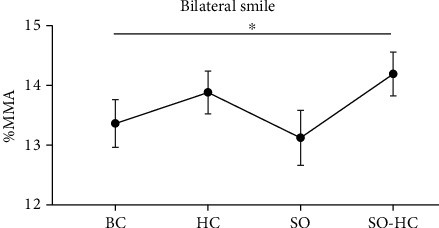
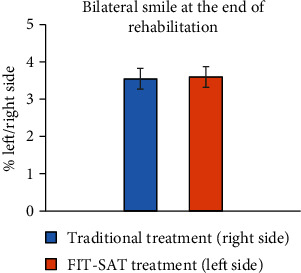
Method: A pre- and postsurgery longitudinal design was adopted to study the efficacy of FIT-SAT. Four patients with bilateral facial nerve paralysis (Moebius syndrome) were included. They underwent two surgeries with free muscle transfers, one year apart from each other. The side of the face first operated on was rehabilitated with the traditional treatment, while the second side was rehabilitated with FIT-SAT. The FIT-SAT treatment includes video clips of an actor performing a unilateral or a bilateral smile to be imitated (FIT condition). In addition to this, while smiling, the participants close their hand in order to exploit the overlapped cortical motor representation of the hand and the mouth, which may facilitate the synergistic activity of the two effectors during the early phases of recruitment of the transplanted muscles (SAT). The treatment was also aimed at avoiding undesired movements such as teeth grinding. Discussion. Results support FIT-SAT as a viable alternative for smile rehabilitation after free muscle transfer. We propose that the treatment potentiates the effect of smile observation by activating the same neural structures responsible for the execution of the smile and therefore by facilitating its production. Closing of the hand induces cortical recruitment of hand motor neurons, recruiting the transplanted muscles, and reducing the risk of associating other unwanted movements such as teeth clenching to the smile movements.
Copyright © 2021 Elisa De Stefani et al.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
