

Classification and analysis of outcome predictors in non-critically ill COVID-19 patients
- PMID: 33835685
- PMCID: PMC8250466
- DOI: 10.1111/imj.15140
Classification and analysis of outcome predictors in non-critically ill COVID-19 patients
Abstract
Background: Early detection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)-infected patients who could develop a severe form of COVID-19 must be considered of great importance to carry out adequate care and optimise the use of limited resources.
Aims: To use several machine learning classification models to analyse a series of non-critically ill COVID-19 patients admitted to a general medicine ward to verify if any clinical variables recorded could predict the clinical outcome.
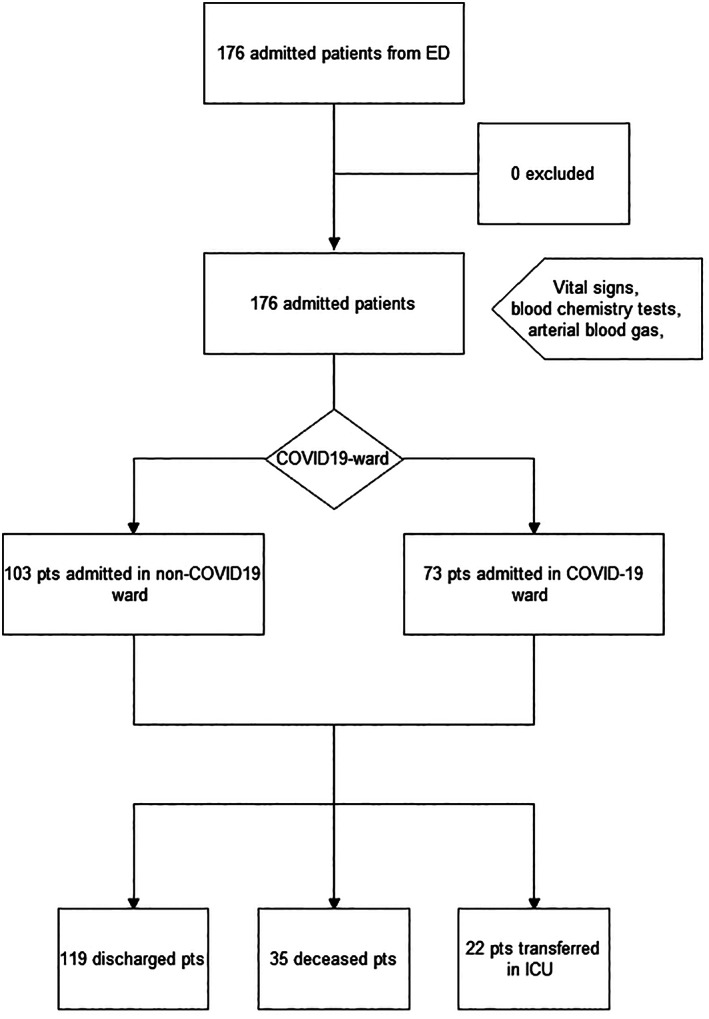
Methods: We retrospectively analysed non-critically ill patients with COVID-19 admitted to the general ward of the hospital in Pordenone from 1 March 2020 to 30 April 2020. Patients' characteristics were compared based on clinical outcomes. Through several machine learning classification models, some predictors for clinical outcome were detected.
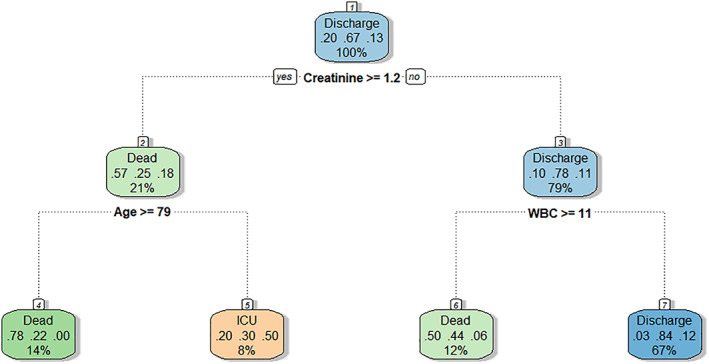
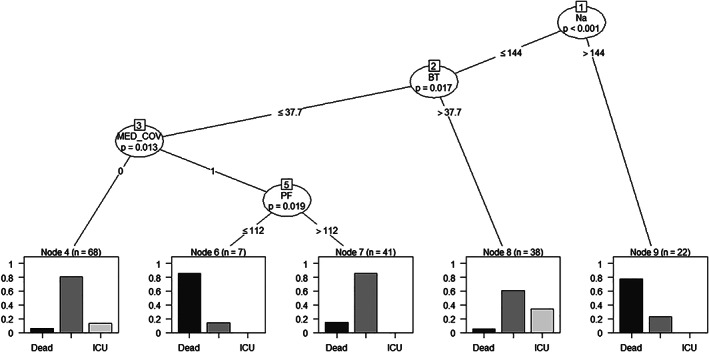
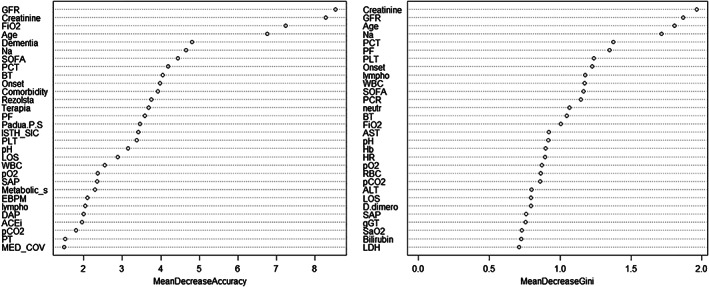
Results: In the considered period, we analysed 176 consecutive patients admitted: 119 (67.6%) were discharged, 35 (19.9%) dead and 22 (12.5%) were transferred to intensive care unit. The most accurate models were a random forest model (M2) and a conditional inference tree model (M5) (accuracy = 0.79; 95% confidence interval 0.64-0.90, for both). For M2, glomerular filtration rate and creatinine were the most accurate predictors for the outcome, followed by age and fraction-inspired oxygen. For M5, serum sodium, body temperature and arterial pressure of oxygen and inspiratory fraction of oxygen ratio were the most reliable predictors.
Conclusions: In non-critically ill COVID-19 patients admitted to a medical ward, glomerular filtration rate, creatinine and serum sodium were promising predictors for the clinical outcome. Some factors not determined by COVID-19, such as age or dementia, influence clinical outcomes.
Keywords: COVID-19; machine learning; non-critically ill; prediction.
© 2021 Royal Australasian College of Physicians.
Figures
Similar articles
-
Machine learning decision tree algorithm role for predicting mortality in critically ill adult COVID-19 patients admitted to the ICU.J Infect Public Health. 2022 Jul;15(7):826-834. doi: 10.1016/j.jiph.2022.06.008. Epub 2022 Jun 17. J Infect Public Health. 2022. PMID: 35759808 Free PMC article.
-
Clinical Characteristics and Predictors of 28-Day Mortality in 352 Critically Ill Patients with COVID-19: A Retrospective Study.J Epidemiol Glob Health. 2021 Mar;11(1):98-104. doi: 10.2991/jegh.k.200928.001. Epub 2020 Oct 3. J Epidemiol Glob Health. 2021. PMID: 33095982 Free PMC article.
-
Clinical and therapeutic outcomes of COVID-19 intensive care units (ICU) patients: a retrospective study in Ghana.Pan Afr Med J. 2021 Feb 2;38:107. doi: 10.11604/pamj.2021.38.107.27131. eCollection 2021. Pan Afr Med J. 2021. PMID: 33912277 Free PMC article.
-
Post-infectious and post-acute sequelae of critically ill adults with COVID-19.PLoS One. 2021 Jun 17;16(6):e0252763. doi: 10.1371/journal.pone.0252763. eCollection 2021. PLoS One. 2021. PMID: 34138871 Free PMC article.
-
Universal screening for SARS-CoV-2 infection: a rapid review.Cochrane Database Syst Rev. 2020 Sep 15;9(9):CD013718. doi: 10.1002/14651858.CD013718. Cochrane Database Syst Rev. 2020. PMID: 33502003 Free PMC article.
Cited by
-
Clinical characteristics and analysis of risk factors for disease progression of patients with SARS-CoV-2 Omicron variant infection: A retrospective study of 25207 cases in a Fangcang hospital.Front Cell Infect Microbiol. 2022 Oct 31;12:1009894. doi: 10.3389/fcimb.2022.1009894. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 36389157 Free PMC article.
-
Chromogranin A plasma levels predict mortality in COVID-19.PLoS One. 2022 Apr 25;17(4):e0267235. doi: 10.1371/journal.pone.0267235. eCollection 2022. PLoS One. 2022. PMID: 35468164 Free PMC article.
-
Role of MR-proADM and Monocyte CD169 in Predicting In-Hospital and 60-Day Mortality in COVID-19 Patients.Clin Pathol. 2024 Dec 16;17:2632010X241304958. doi: 10.1177/2632010X241304958. eCollection 2024 Jan-Dec. Clin Pathol. 2024. PMID: 39691491 Free PMC article.
-
Challenges in the Differential Diagnosis of COVID-19 Pneumonia: A Pictorial Review.Diagnostics (Basel). 2022 Nov 16;12(11):2823. doi: 10.3390/diagnostics12112823. Diagnostics (Basel). 2022. PMID: 36428883 Free PMC article. Review.
-
A simple prognostic score based on troponin and presepsin for COVID-19 patients admitted to the emergency department: a single-center pilot study.Acta Biomed. 2021 Sep 2;92(4):e2021233. doi: 10.23750/abm.v92i4.11479. Acta Biomed. 2021. PMID: 34487072 Free PMC article.
References
-
- World Health Organisation (WHO) . WHO announces COVID‐19 outbreak a pandemic. Geneva, Switzerland: WHO; 2020. [cited 2020 Jul 11]. Available from https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus...
-
- Du Y, Tu L, Zhu P, Mu M, Wang R, Yang P, Wang X, Hu C, Ping R, Hu P, Li T, Cao F, Chang C, Hu Q, Jin Y, Xu G. Clinical Features of 85 Fatal Cases of COVID‐19 from Wuhan. A Retrospective Observational Study. American Journal of Respiratory and Critical Care Medicine. 2020; 201: 1372–1379. 10.1164/rccm.202003-0543oc. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
