

Clinical characteristics and survival outcomes of malignant struma ovarii confined to the ovary
- PMID: 33836675
- PMCID: PMC8033663
- DOI: 10.1186/s12885-021-08118-7
Clinical characteristics and survival outcomes of malignant struma ovarii confined to the ovary
Abstract
Background: Malignant struma ovarii (MSO) is a unique type of ovarian malignancy that data on the survival outcome is limited and management strategy remains controversial due to its extreme rarity.
Methods: To investigate the clinical characteristics and treatment options in patients with MSO confined to the ovary, while also evaluating the recurrent-free survival (RFS) and overall survival (OS) rate in this population, a retrospective study was conducted. One hundred twenty-five cases of MSO confined to the ovary were enrolled and their clinical characteristics, treatment strategies, and results of follow-up were analyzed. OS and RFS were assessed by Kaplan-Meier analyses and Cox regression models.
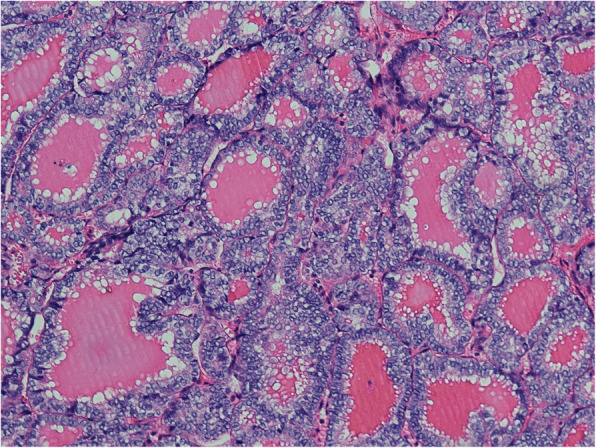
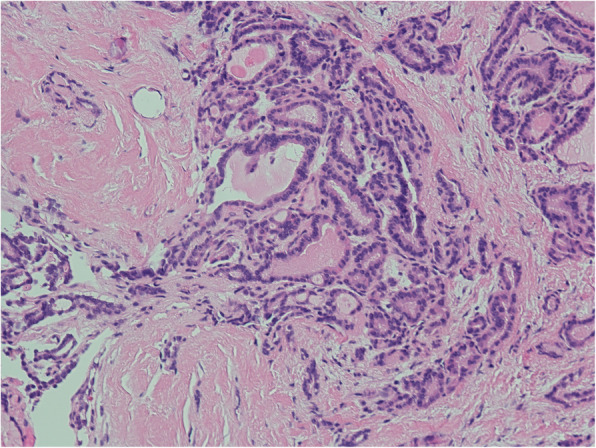
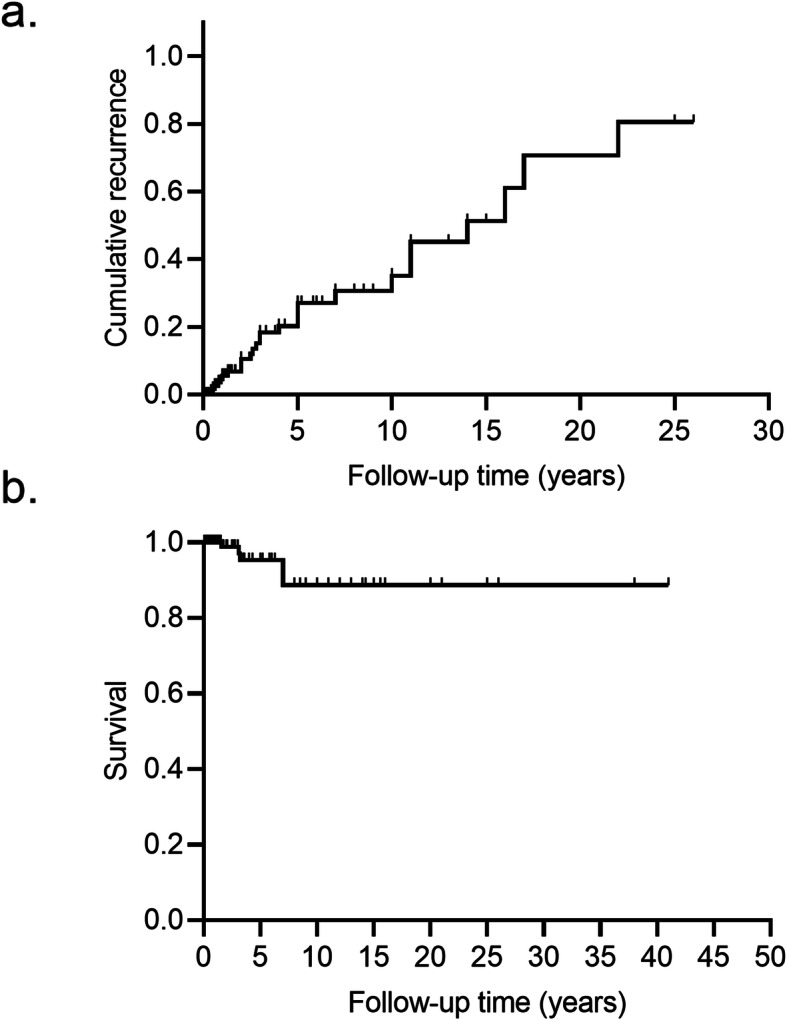
Results: The most common pathological subtype in this cohort was papillary carcinoma (44.8%). Other reported subtypes, in order of prevalence, were follicular variant of papillary carcinoma, follicular carcinoma, and mixed follicular-papillary carcinoma. Surgical treatment options varied in this cohort that 8.0% of the patients received ovarian cystectomy, 33.6% underwent unilateral salpingo-oophorectomy (USO), 5.6% received bilateral salpingo-oophorectomy (BSO), 21.6% received total abdominal hysterectomy with BSO (TAH/BSO), and 17.6% were treated with debulking surgery; 20.0% of them received radioiodine therapy (RAI). Twenty-seven patients experienced recurrence with a median RFS of 14.0 years (95% confidence interval [CI], 9.5-18.5). The 5-year and 10-year recurrent rate were 27.1, 35.2%, respectively. Eight patients died during follow-up, with five attributed to MSO; the 5-year, 10-year, and 20-year OS rate was 95.3, 88.7 and 88.7%, respectively. However, the univariate and multivariate Cox regression showed no potential risk factor for RFS and OS.
Conclusion: Patients with MSO confined to the ovary had an excellent survival outcome, despite varied treatment strategies, and the recurrent rate was relatively high. We recommend USO as the preferred surgical option in this population since more aggressive surgery does not improve outcomes and the benefits of RAI are uncertain.
Keywords: Adjuvant therapy; Malignant struma ovarii; Prognosis; Surgery; Thyroid carcinoma.
Conflict of interest statement
The authors declare that they have no conflict of interests.
Figures

References
-
- Fujiwara S, Tsuyoshi H, Nishimura T, Takahashi N, Yoshida Y. Precise preoperative diagnosis of struma ovarii with pseudo-Meigs’ syndrome mimicking ovarian cancer with the combination of 131I scintigraphy and 18F–FDG PET: case report and review of the literature. J Ovarian Res. 2018;11(1):11. doi: 10.1186/s13048-018-0383-2. - DOI - PMC - PubMed
-
- Hanby A, Walker C. Pathology and Genetics: Tumours of the Breast and Female Genital Organs. WHO Classification of Tumours series - volume IV. Lyon: IARC Press. Breast Cancer Res; 2004. p. 133.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
