

Is the "Brainwork Intervention" effective in reducing sick leave for non-permanent workers with psychological problems? Results of a controlled clinical trial
- PMID: 33836711
- PMCID: PMC8034165
- DOI: 10.1186/s12889-021-10704-0
Is the "Brainwork Intervention" effective in reducing sick leave for non-permanent workers with psychological problems? Results of a controlled clinical trial
Abstract
Background: Both the presence of psychological problems and the absence of an employment contract are related to long-term sickness absence, prolonged work disability and unemployment. Studies researching the effectiveness of return-to-work interventions on these non-permanent workers, including unemployed and temporary agency workers and workers with an expired fixed-term contract, are lagging behind. Therefore, a return-to-work intervention called "Brainwork" was developed. The aim of this study was to assess the effectiveness of the 'Brainwork Intervention' in reducing the duration of sick leave compared to usual care over a 12-month follow-up.
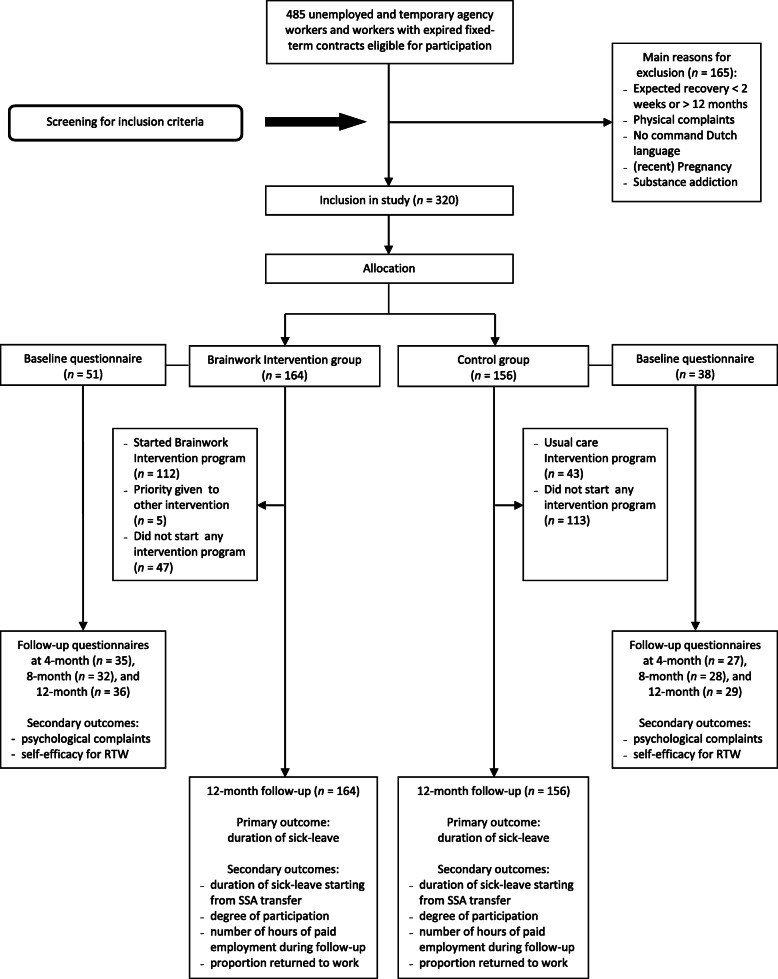
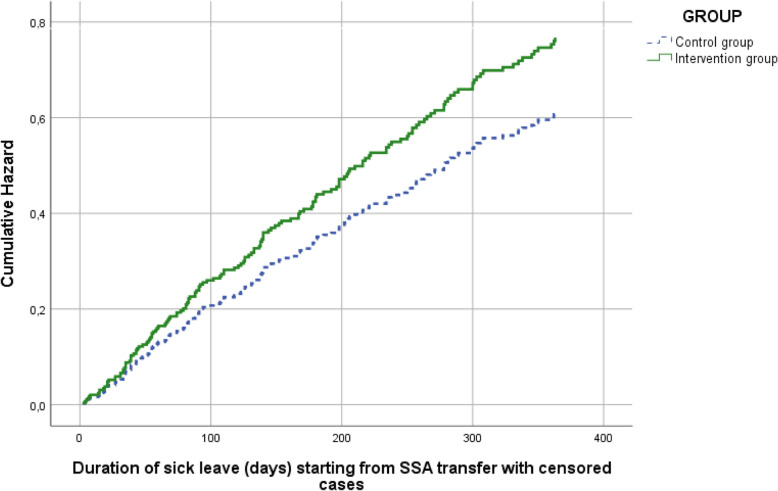
Methods: In a multicenter controlled clinical trial, using a quasi-randomization procedure, we compared the Brainwork Intervention (n = 164) to usual care (n = 156). The primary outcome was the duration of sick leave. Secondary outcomes were the duration of sick leave starting from Social Security Agency transfer; the proportion of workers returned to work; the number of hours of paid employment during the follow-up period; the degree of worker participation; the level of psychological complaints; and the self-efficacy for return to work. Protocol adherence (Brainwork Intervention) was considered sufficient when at least three of the five protocol steps were followed. Cox regressions, linear and ordinal regression, and Mixed Model analyses were performed.
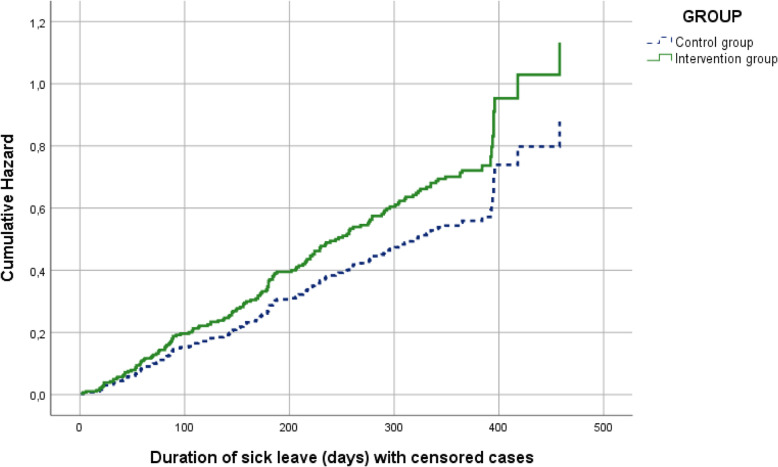
Results: All 320 participants were analyzed. The Brainwork Intervention resulted in a non-significant reduction of the duration of sick leave compared to usual care (269 days versus 296 days; HR = 1.29; 95% CI 0.94-1.76; p = 0.11). For those working (46%) during the 12-month follow-up, the mean number of hours of paid employment was non-significantly higher in the usual care group (682 h versus 493 h; p = 0.053). No significant differences were found for other secondary outcomes. Protocol adherence was 10%.
Conclusions: The Brainwork Intervention as performed with a low protocol adherence did not result in a significant reduction of the duration of sick leave compared to usual care. It remains unclear what the results would have been if the Brainwork Intervention had been executed according to protocol.
Trial registration: The Netherlands Trial Register (NTR); NTR3976 (old registration number NTR4190). Registered September 27th 2013.
Keywords: Counselling; Intervention; Participation; Psychological problems; Return-to-work; Sick leave; Unemployment; Vocational rehabilitation.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- OECD . Sickness, disability and work: breaking the barriers. Paris: OECD Publishing; 2010.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
