

Capacity and site readiness for hypertension control program implementation in the Federal Capital Territory of Nigeria: a cross-sectional study
- PMID: 33836719
- PMCID: PMC8034094
- DOI: 10.1186/s12913-021-06320-8
Capacity and site readiness for hypertension control program implementation in the Federal Capital Territory of Nigeria: a cross-sectional study
Abstract
Background: Nigeria faces an increase in the burden of non-communicable diseases (NCDs), including cardiovascular diseases (CVDs), leading to an estimated 29% of all deaths in the country. Nigeria has an estimated hypertension prevalence ranging from 25 to 40% of her adult population. Despite this high burden, awareness (14-30%), treatment (< 20%), and control (9%) rates of hypertension are low in Nigeria. Against this backdrop, we sought to perform capacity and readiness assessments of public Primary Healthcare Centers (PHCs) to inform Nigeria's system-level hypertension control program's implementation and adaptation strategies.
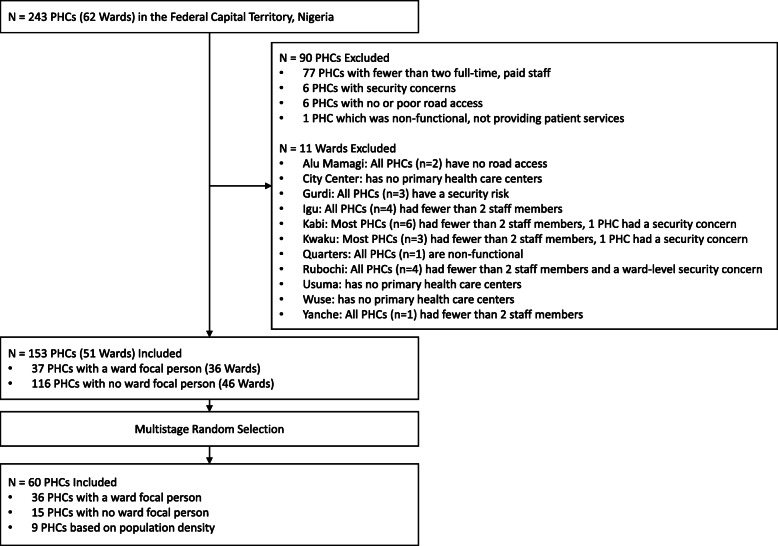
Methods: The study employed a multi-stage sampling to select 60 from the 243 PHCs in the Federal Capital Territory (FCT) of Nigeria. The World Health Organization (WHO) Service Availability and Readiness Assessment was adapted to focus on hypertension diagnosis and treatment and was administered to PHC staff from May 2019 - October 2019. Indicator scores for general and cardiovascular service readiness were calculated based on the proportion of sites with available amenities, equipment, diagnostic tests, and medications.
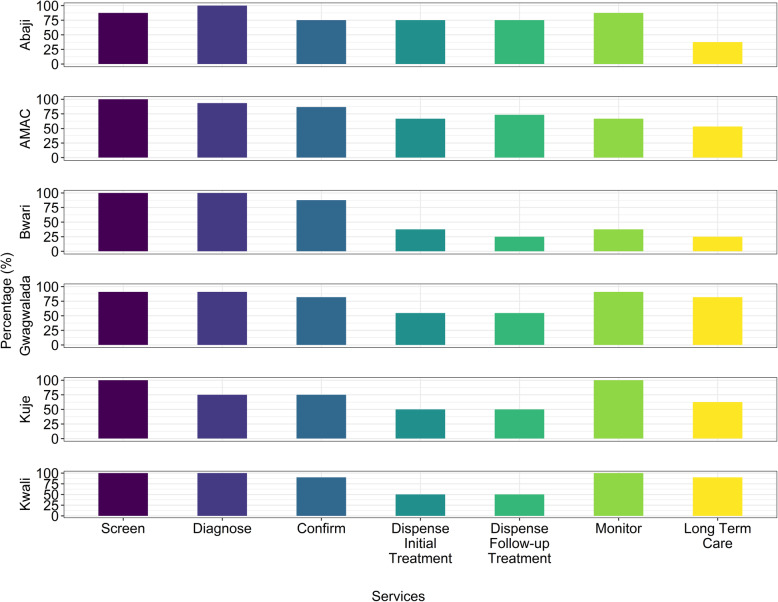
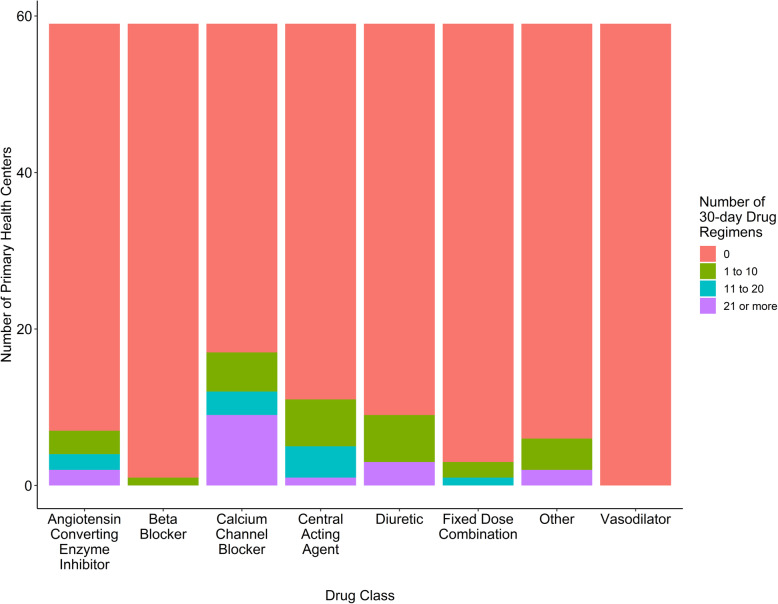
Results: Median (interquartile range [IQR]) number of full-time staff was 5 (3-8), and were predominantly community health extension workers (median = 3 [IQR 2-5]). Few sites (n = 8; 15%) received cardiovascular disease diagnosis and management training within the previous 2 years, though most had sufficient capacity for screening (n = 58; 97%), diagnosis (n = 56; 93%), and confirmation (n = 50; 83%) of hypertension. Few PHCs had guidelines (n = 7; 13%), treatment algorithms (n = 3; 5%), or information materials (n = 1; 2%) for hypertension. Most sites (n = 55; 92%) had one or more functional blood pressure apparatus. All sites relied on paper records, and few had a functional computer (n = 10; 17%) or access to internet (n = 5; 8%). Despite inclusion on Nigeria's essential medicines list, 35 (59%) PHCs had zero 30-day treatment regimens of any blood pressure-lowering medications in stock.
Conclusions: This first systematic assessment of capacity and readiness for a system-level hypertension control program within the FCT of Nigeria demonstrated implementation feasibility based on the workforce, equipment, and paper-based information systems, but a critical need for essential medicine supply strengthening, health-worker training, and protocols for hypertension treatment and control in Nigeria.
Keywords: Capacity; Hypertension; Nigeria; Primary health care; Readiness.
Conflict of interest statement
Dr. Huffman reports grants from American Heart Association, Verily, AstraZeneca, personal fees from American Medical Association, outside the submitted work. The George Institute for Global Health has a patent, license, and has received investment funding with intent to commercialize fixed-dose combination therapy through its social enterprise business, George Medicines. All other authors declare that they have no competing interests.
Figures
References
-
- Reliefweb. Nigeria Fulfils Commitment, launches Plan for the Prevention and Control of Non-Communicable Diseases: United Nations Office for the Coordination of Humanitarian Affairs (OCHA) services; 2019. https://reliefweb.int/report/nigeria/nigeria-fulfils-commitment-launches.... Accessed 16 Apr 2020
-
- Whelton PK, Carey RM, Aronow WS, Casey DE, Jr, Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, MacLaughlin EJ, Muntner P, Ovbiagele B, Smith SC, Jr, Spencer CC, Stafford RS, Taler SJ, Thomas RJ, Williams KA, Sr, Williamson JD, Wright JT., Jr 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. J Am Coll Cardiol. 2018;71(19):2199–2269. doi: 10.1161/HYP.0000000000000066. - DOI - PubMed
-
- Federal Ministry of Health (FMoH) Nigeria . National Multi-Sectoral Action Plan for the Prevention and Control of Non-Communicable Diseases (2019–2025) 2019.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
