

Gender Differences in Treatment Allocation and Survival of Advanced Gastroesophageal Cancer: A Population-Based Study
- PMID: 33837791
- PMCID: PMC8562959
- DOI: 10.1093/jnci/djab075
Gender Differences in Treatment Allocation and Survival of Advanced Gastroesophageal Cancer: A Population-Based Study
Abstract
Background: Biological sex and gender have been reported to affect incidence and overall survival (OS) of curatively treated gastroesophageal cancer. The aim of this study was to compare palliative treatment allocation and OS between women and men with advanced gastroesophageal cancer.
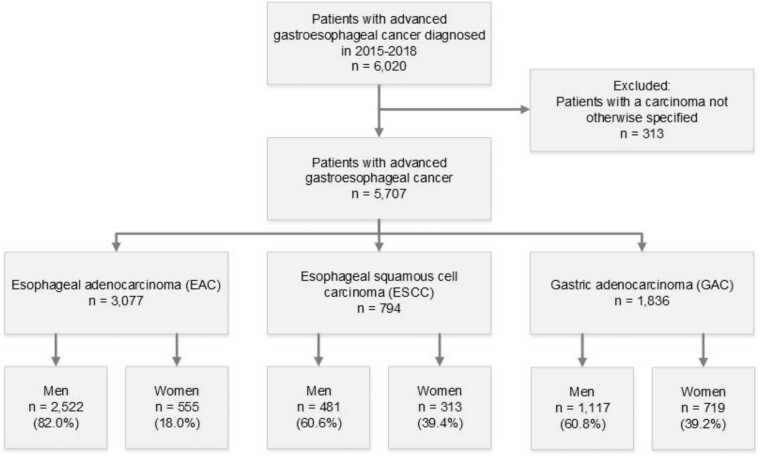
Methods: Patients with an unresectable or metastatic esophageal (including cardia) adenocarcinoma (EAC) or squamous cell carcinoma (ESCC) or gastric adenocarcinoma (GAC) diagnosed in 2015-2018 were identified in the Netherlands Cancer Registry. Treatment allocation was compared using χ2 tests and multivariable logistic regression analyses, and OS using the Kaplan-Meier method with log-rank test and Cox proportional hazards analysis. All statistical tests were 2-sided.
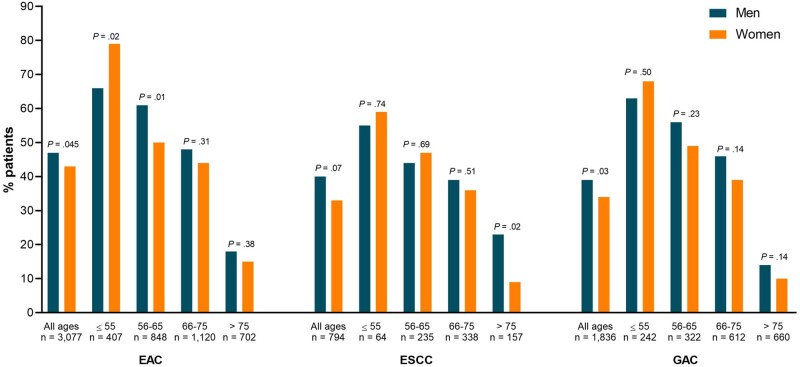
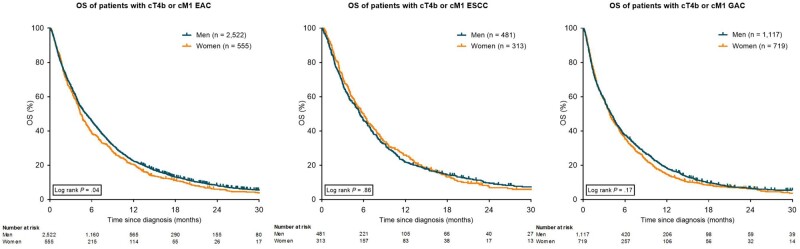
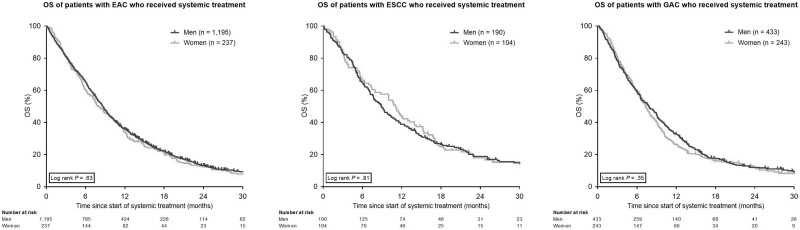
Results: Of patients with EAC (n = 3077), ESCC (n = 794), and GAC (n = 1836), 18.0%, 39.4%, and 39.1% were women, respectively. Women less often received systemic treatment compared with men for EAC (42.7% vs 47.4%, P = .045) and GAC (33.8% vs 38.8%, P = .03) but not for ESCC (33.2% vs 39.5%, P = .07). Women had a lower probability of receiving systemic treatment for GAC in multivariable analyses (odds ratio [OR] = 0.79, 95% confidence interval [CI] = 0.62 to 1.00) but not for EAC (OR = 0.86, 95% CI = 0.69 to 1.06) and ESCC (OR = 0.81, 95% CI = 0.57 to 1.14). Median OS was lower in women with EAC (4.4 vs 5.2 months, P = .04) but did not differ after adjustment for patient and tumor characteristics and systemic treatment administration.
Conclusions: We observed statistically significant and clinically relevant gender differences in systemic treatment administration and OS in advanced gastroesophageal cancer. Causes of these disparities may be sex based (ie, related to tumor biology) as well as gender based (eg, related to differences in treatment choices).
© The Author(s) 2021. Published by Oxford University Press.
Figures
References
-
- Netherlands Comprehensive Cancer Organization (IKNL). Dutch Cancer Figures.
-
- Ferlay J, Colombet M, Soerjomataram I, et al.Cancer incidence and mortality patterns in Europe: estimates for 40 countries and 25 major cancers in 2018. Eur J Cancer. 2018;103:356–387. - PubMed
-
- Siegel RL, Miller KD, Jemal A.. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7–30. - PubMed
-
- Najari BB, Rink M, Li PS, et al.Sex disparities in cancer mortality: the risks of being a man in the United States. J Urol. 2013;189(4):1470–1474. - PubMed
-
- Özdemir BC, Csajka C, Dotto GP, Wagner AD.. Sex differences in efficacy and toxicity of systemic treatments: an undervalued issue in the era of precision oncology. J Clin Oncol. 2018;36(26):2680–2683. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
