

First but not second postoperative day growth hormone assessments as early predictive tests for long-term acromegaly persistence
- PMID: 33837920
- PMCID: PMC8502138
- DOI: 10.1007/s40618-021-01553-0
First but not second postoperative day growth hormone assessments as early predictive tests for long-term acromegaly persistence
Abstract
Purpose: Postoperative assessment of acromegaly activity is typically performed at least 3 months after neurosurgery (NS). Few studies have evaluated the use of early postoperative growth hormone (GH) levels as a test to predict short- and long-term remission of acromegaly. Our objective was to evaluate the diagnostic performance of serum random GH on a postoperative day one (D1-rGH) and two (D2-rGH), particularly in predicting long-term disease persistence.
Materials and methods: Forty-one subjects with acromegaly who were undergoing NS were enrolled (mean age ± SD 47.4 ± 13.1 years at diagnosis; women 54%; macroadenomas 71%). The final assessment of disease activity was performed one year after NS. ROC curves were used to evaluate the diagnostic performance of D1-rGH and D2-rGH.
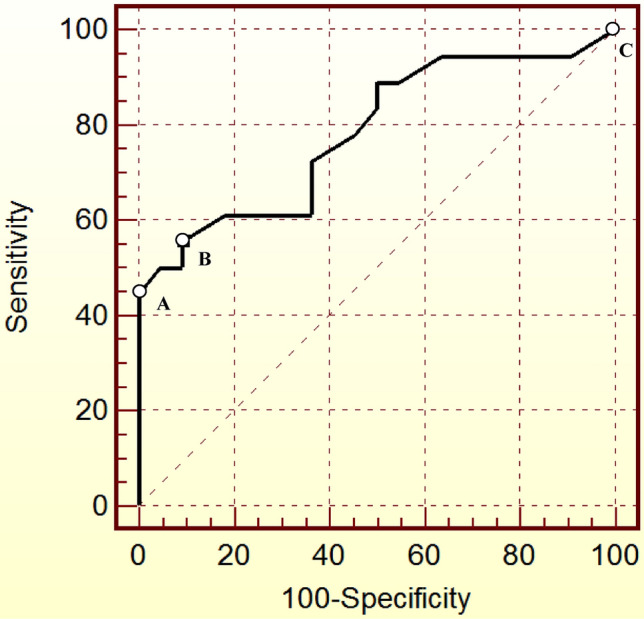
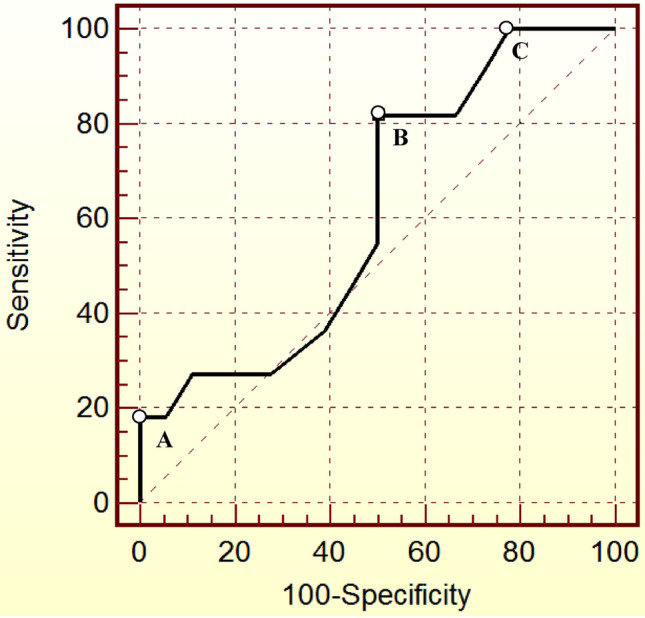
Results: After a 1-year follow-up, the overall remission rate was 55%. ROC analysis identified an optimal D1-rGH cut-off value of 2.1 ng/mL for diagnosing long-term disease persistence (55.6% SE; 90.9% SP). The cut-off point became 2.5 ng/mL after maximizing specificity for disease persistence (yielding a 100% positive predictive value) and 0.3 ng/mL after maximizing sensitivity for disease remission. The optimal D2-rGH cut-off value was 0.6 ng/mL (81.8% SE; 50% SP); the cut-off point became 2.9 ng/mL after maximizing specificity and 0.1 ng/mL after maximizing sensitivity, with no clinical utility.
Conclusions: D1-rGH could be a highly specific test for the early diagnosis of long-term acromegaly persistence, which is predicted by a value > 2.5 ng/mL with a great degree of certainty. The diagnostic performance of D2-rGH was insufficient. Further research is required to validate these preliminary results prior to modifying the postoperative management of acromegaly.
Keywords: Acromegaly; Disease persistence; Early prediction; Growth hormone.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Starke RM, Raper DM, Payne SC, Vance ML, Oldfield EH, Jane JA. Endoscopic vs microsurgical transsphenoidal surgery for acromegaly: outcomes in a concurrent series of patients using modern criteria for remission. J Clin Endocrinol Metab. 2013;98(8):3190–3198. doi: 10.1210/jc.2013-1036. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
