

doi: 10.1002/ajh.26185.
Epub 2021 Apr 24.
Age-dependent and gender-dependent antibody responses against SARS-CoV-2 in health workers and octogenarians after vaccination with the BNT162b2 mRNA vaccine
Affiliations
- PMID: 33837984
- PMCID: PMC8250071
- DOI: 10.1002/ajh.26185
Item in Clipboard
Age-dependent and gender-dependent antibody responses against SARS-CoV-2 in health workers and octogenarians after vaccination with the BNT162b2 mRNA vaccine
Am J Hematol.
.
No abstract available
Figures
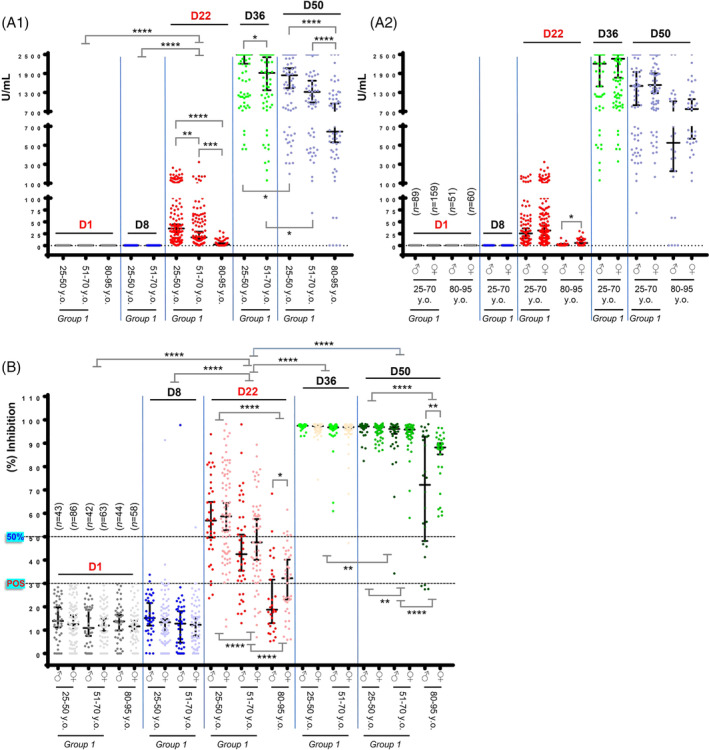
Anti‐Spike‐RBD and neutralizing antibodies (NAbs) against SARS‐CoV‐2 in health workers and octogenarians after vaccination with the BNT162b2 mRNA vaccine. (A1) Anti‐Spike‐RBD IgG antibodies in donors of group one increased on D22 (day of second vaccination), reached a plateau 2 weeks after the second dose of the vaccine (D36; median U/mL for ages 25–50, 2500, and for ages 51–70, 1918.5) and started to decline at D50 (D50; median U/mL for ages 25–50, 1844, and for ages 51–70, 1319). The efficacy of the vaccine‐mediated anti‐Spike‐RBD IgG immune responses is age‐dependent as evident on both D22 (median U/mL for ages 25–50, 35.94; for ages 51–70, 17.36; and for octogenarians, 2.28) and on D50 (median U/mL for ages 25–50, 1844; for ages 51–70, 1319; and for octogenarians, 644.5). (A2) Development of anti‐Spike‐RBD IgG antibodies on D22 tended to be more intense in females vs males in the younger ages (males, median U/mL, 25.55; females, median U/mL, 31.46) and was significant in octogenarians (males, median U/mL, 0.793; females, median U/mL, 5.36). On D50, the noted difference for male vs female octogenarians (males, median U/mL, 526; females, median U/mL, 778) did not reach statistical significance. All positive for anti‐Spike‐RBD IgG antibodies participants on D1 have been removed (see text) to show only [n values in (A2)] the vaccine‐mediated effects; values are not paired with those shown in B. Median ages per group are reported in B,; for D1, D8 vs D36 or D50 in (A1) p < .001 (not indicated). (B) NAbs in donors of group 1 increased on D22, plateaued 2 weeks after the second dose of the vaccine (D36) [median NAbs (%) inhibition (all donors), 97.22] and remained (with a slight decline) at high levels on D50 [median NAbs (%) inhibition (all donors), 96.62] indicating that NAbs are likely more durable vs anti‐RBD IgGs (see A1) following BNT162b2 vaccination. On D22 the kinetics of accumulating NAbs (%) inhibition titers were age dependent as evident by comparing donors aged 25–50 [median NAbs (%) inhibition, 57.55] vs donors aged 51–70 (median NAbs (%) inhibition, 44.39) and for both age groups vs octogenarians (median NAbs (%) inhibition, 23.20); similar age‐dependent readouts were observed on D50. Immune responses tended to be more robust in females vs males reaching statistical significance on D22 and D50 in octogenarians, suggesting gender dependent humoral immune responses, at least in the elderly individuals. To demonstrate only the vaccine effect, all positive for NAbs donors (see text) on D1 have been removed. Shown n values denote the number of initially enrolled (negative for NAbs) participants in this on‐going study. For D1 or D8 vs D36, D50, p < .001 (not indicated). 25–50 years old.: ♂ Median Age: 39, ♀ Median Age: 39; 51–70 years old: ♂ Median Age: 60, ♀ Median Age: 59; 80–95 years old: ♂ Median Age: 84.5, ♀: Median Age: 85. In both A,B, * p ANOVA <.05, ** p‐ANOVA <.01, *** p‐ANOVA <.001, **** p‐ANOVA <.001). Plotted are Median values with 95% Confidence Interval (GraphPad Prism 7)
References
-
- Tan CW, Chia WN, Qin X, et al. A SARS‐CoV‐2 surrogate virus neutralization test based on antibody‐mediated blockage of ACE2–spike protein–protein interaction. Nat Biotechnol. 2020;38(9):1073‐1078. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous