

Ready-to-Use Therapeutic Food (RUTF) Containing Low or No Dairy Compared to Standard RUTF for Children with Severe Acute Malnutrition: A Systematic Review and Meta-Analysis
- PMID: 33838044
- PMCID: PMC8483958
- DOI: 10.1093/advances/nmab027
Ready-to-Use Therapeutic Food (RUTF) Containing Low or No Dairy Compared to Standard RUTF for Children with Severe Acute Malnutrition: A Systematic Review and Meta-Analysis
Abstract
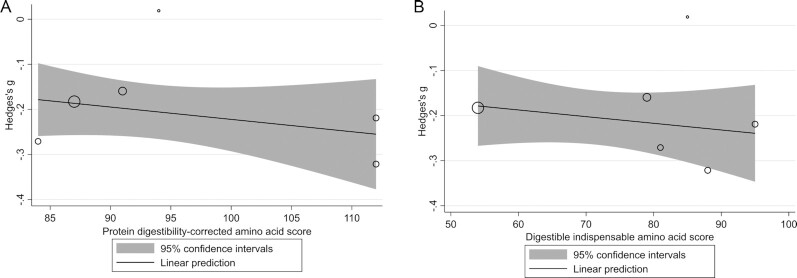
Ready-to-use therapeutic food (RUTF) containing less dairy may be a lower-cost treatment option for severe acute malnutrition (SAM). The objective was to understand the effectiveness of RUTF containing alternative sources of protein (nondairy), or <50% of protein from dairy products, compared with standard RUTF in children with SAM. The Cochrane Library, MEDLINE, Embase, CINAHL, and Web of Science were searched using terms relating to RUTF. Studies were eligible if they included children with SAM and evaluated RUTF with <50% of protein from dairy products compared with standard RUTF. Meta-analysis and meta-regression were completed to assess the effectiveness of intervention RUTF on a range of child outcomes. The quality of the evidence across outcomes was assessed using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach. A total of 5868 studies were identified, of which 8 articles of 6 studies met the inclusion criteria evaluating 7 different intervention RUTF recipes. Nondairy or lower-dairy RUTF showed less weight gain (standardized mean difference: -0.20; 95% CI: -0.26, -0.15; P < 0.001), lower recovery (relative risk ratio: 0.93; 95% CI: 0.87, 1.00; P = 0.046), and lower weight-for-age z scores (WAZ) near program discharge (mean difference: -0.10; 95% CI: -0.20, 0.0; P = 0.047). Mortality, time to recovery, default (consecutive absences from outpatient therapeutic feeding program visits), nonresponse, and other anthropometric measures did not differ between groups. The certainty of evidence was high for weight gain and ranged from very low to moderate for other outcomes. RUTF with lower protein from dairy or dairy-free RUTF may not be as effective as standard RUTF for treatment of children with SAM based on weight gain, recovery, and WAZ evaluated using meta-analysis, although further research is required to explore the potential of alternative formulations. This review was registered at https://www.crd.york.ac.uk/prospero/ as CRD42020160762.
Keywords: CMAM; DIAAS; PDCAAS; meta-analysis; meta-regression; network meta-analysis; protein quality; severe acute malnutrition.
© The Author(s) 2021. Published by Oxford University Press on behalf of the American Society for Nutrition.
Figures







Comment in
-
Reply to I Potani et al.Adv Nutr. 2022 Jun 1;13(3):970-972. doi: 10.1093/advances/nmac024. Adv Nutr. 2022. PMID: 35641237 Free PMC article. No abstract available.
References
-
- World Health Organization . Management of severe malnutrition: a manual for physicians and other senior health workers. Geneva (Switzerland): World Health Organization; 1999.
-
- World Health Organization . Community-based management of severe acute malnutrition: a joint statement by the World Health Organization, the World Food Programme, the United Nations System Standing Committee on Nutrition and the United Nations Children's Fund. Geneva (Switzerland): World Health Organization; 2007.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
