

A birth population-based survey of preterm morbidity and mortality by gestational age
- PMID: 33838659
- PMCID: PMC8037918
- DOI: 10.1186/s12884-021-03726-4
A birth population-based survey of preterm morbidity and mortality by gestational age
Erratum in
-
Correction to: A birth population-based survey of preterm morbidity and mortality by gestational age.BMC Pregnancy Childbirth. 2021 May 12;21(1):373. doi: 10.1186/s12884-021-03841-2. BMC Pregnancy Childbirth. 2021. PMID: 33980162 Free PMC article. No abstract available.
Abstract
Background: Despite 15-17 millions of annual births in China, there is a paucity of information on prevalence and outcome of preterm birth. We characterized the outcome of preterm births and hospitalized preterm infants by gestational age (GA) in Huai'an in 2015, an emerging prefectural region of China.
Methods: Of 59,245 regional total births, clinical data on 2651 preterm births and 1941 hospitalized preterm neonates were extracted from Huai'an Women and Children's Hospital (HWCH) and non-HWCH hospitals in 2018-2020. Preterm prevalence, morbidity and mortality rates were characterized and compared by hospital categories and GA spectra. Death risks of preterm births and hospitalized preterm infants in the whole region were analyzed with multivariable Poisson regression.
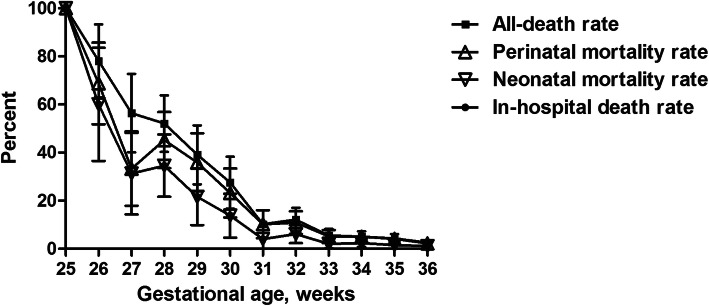
Results: The prevalence of extreme, very, moderate, late and total preterm of the regional total births were 0.14, 0.53, 0.72, 3.08 and 4.47%, with GA-specific neonatal mortality rates being 44.4, 15.8, 3.7, 1.5 and 4.3%, respectively. There were 1025 (52.8% of whole region) preterm admissions in HWCH, with significantly lower in-hospital death rate of inborn (33 of 802, 4.1%) than out-born (23 of 223, 10.3%) infants. Compared to non-HWCH, three-fold more neonates in HWCH were under critical care with higher death rate, including most extremely preterm infants. Significantly all-death risks were found for the total preterm births in birth weight < 1000 g, GA < 32 weeks, amniotic fluid contamination, Apgar-5 min < 7, and birth defects. For the hospitalized preterm infants, significantly in-hospital death risks were found in out-born of HWCH, GA < 32 weeks, birth weight < 1000 g, Apgar-5 min < 7, birth defects, respiratory distress syndrome, necrotizing enterocolitis and ventilation, whereas born in HWCH, antenatal glucocorticoids, cesarean delivery and surfactant use decreased the death risks.
Conclusions: The integrated data revealed the prevalence, GA-specific morbidity and mortality rate of total preterm births and their hospitalization, demonstrating the efficiency of leading referral center and whole regional perinatal-neonatal network in China. The concept and protocol should be validated in further studies for prevention of preterm birth.
Keywords: Birth population; Gestation; Morbidity; Mortality; Preterm; Prevalence; Regional perinatal-neonatal network.
Conflict of interest statement
All the authors have declared no any financial and non-financial competing interests to disclose.
Figures

References
-
- Ancel PY, Goffinet F, EPIPAGE-2 Writing Group. Kuhn P, Langer B, Matis J, et al. Survival and morbidity of preterm children born at 22 through 34 weeks’ gestation in France in 2011: Results of the EPIPAGE-2 cohort study. JAMA Pediatr. 2015;169(3):230–238. doi: 10.1001/jamapediatrics.2014.3351. - DOI - PubMed
-
- Norman M, Hallberg B, Abrahamsson T, Björklund LJ, Domellöf M, Farooqi A, Foyn Bruun C, Gadsbøll C, Hellström-Westas L, Ingemansson F, Källén K, Ley D, Maršál K, Normann E, Serenius F, Stephansson O, Stigson L, Um-Bergström P, Håkansson S. Association between year of birth and 1-year survival among extremely preterm infants in Sweden during 2004-2007 and 2014-2016. JAMA. 2019;321(12):1188–1199. doi: 10.1001/jama.2019.2021. - DOI - PMC - PubMed
-
- Bolisetty S, Legge N, Bajuk B, Lui K, New South Wales and the Australian Capital Territory neonatal intensive care Units' data collection Preterm infant outcomes in New South Wales and the Australian Capital Territory. J Paediatr Child Health. 2015;51(7):713–721. doi: 10.1111/jpc.12848. - DOI - PubMed
-
- Helenius K, Sjörs G, Shah PS, Modi N, Reichman B, Morisaki N, et al. Survival in very preterm infants: an international comparison of 10 national neonatal networks. Pediatrics 2017; 140 (6). pii: e20171264. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
