

Gene-Specific Variation in Colorectal Cancer Surveillance Strategies for Lynch Syndrome
- PMID: 33839100
- PMCID: PMC9330543
- DOI: 10.1053/j.gastro.2021.04.010
Gene-Specific Variation in Colorectal Cancer Surveillance Strategies for Lynch Syndrome
Abstract
Background and aims: Lynch syndrome is associated with pathogenic variants in 4 mismatch repair (MMR) genes that increase lifetime risk of colorectal cancer. Guidelines recommend intensive colorectal cancer surveillance with colonoscopy every 1-2 years starting at age 25 years for all carriers of Lynch syndrome-associated variants, regardless of gene product. We constructed a simulation model to analyze the effects of different ages of colonoscopy initiation and surveillance intervals for each MMR gene (MLH1, MSH2, MSH6, and PMS2) on colorectal cancer incidence and mortality, quality-adjusted life-years, and cost.
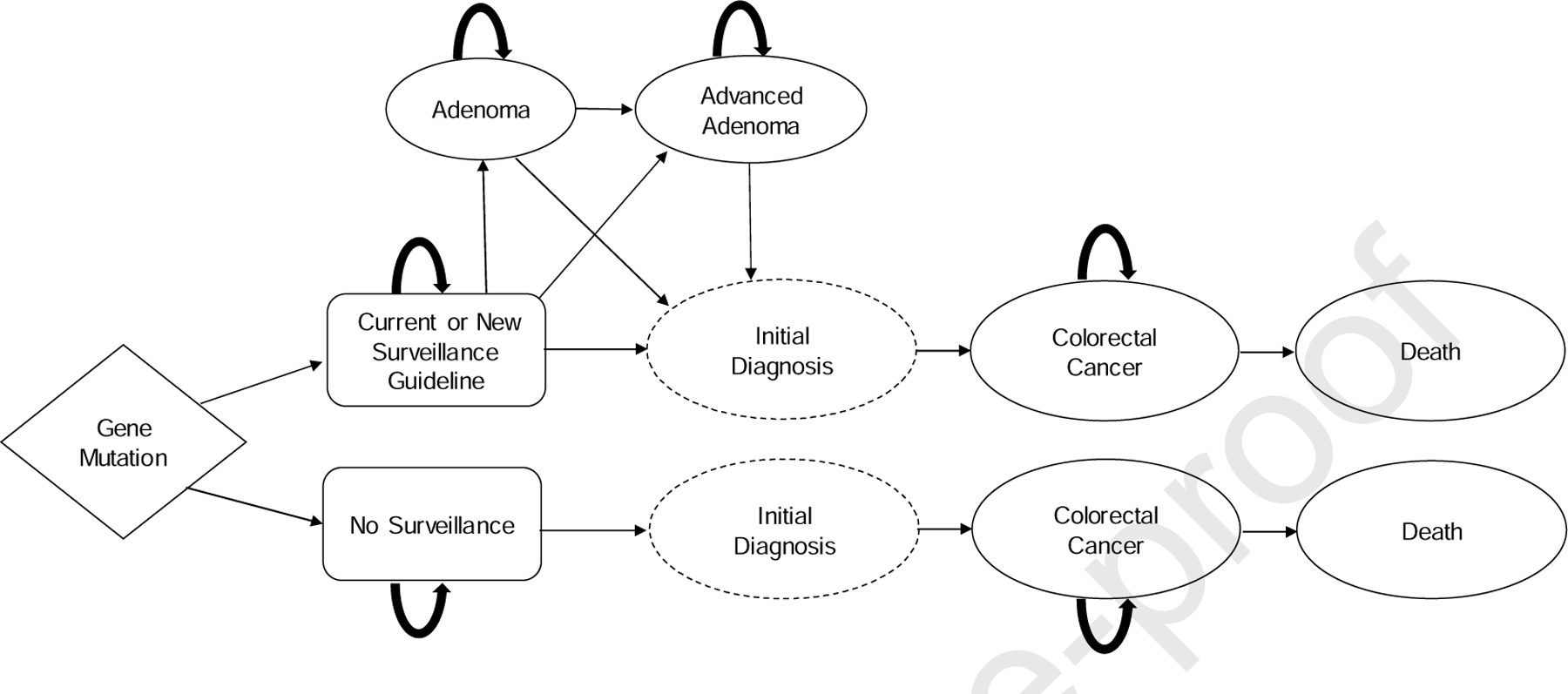
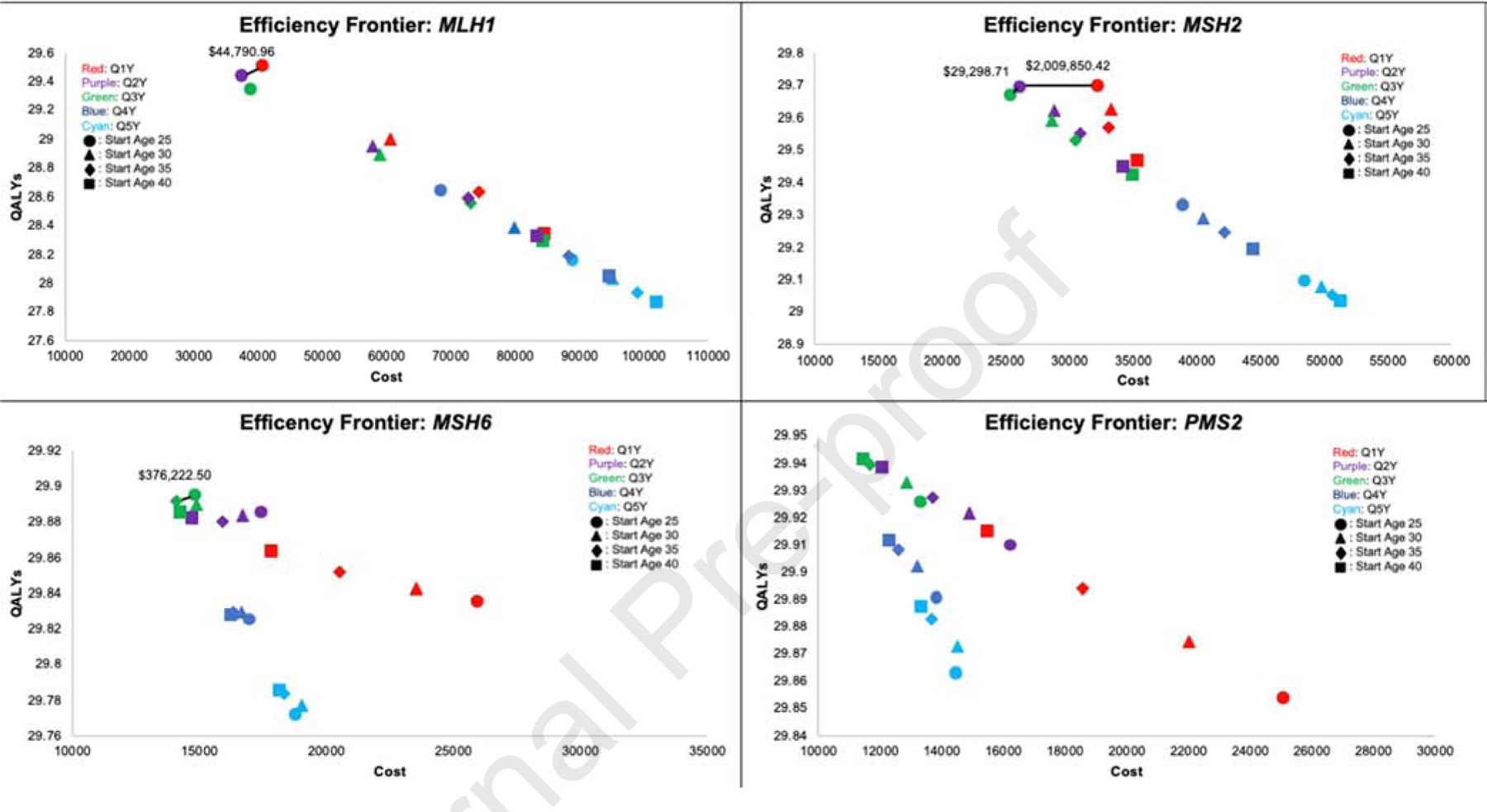
Methods: Using published literature, we developed a Markov simulation model of Lynch syndrome progression for patients with each MMR variant. The model simulated clinical trials of Lynch syndrome carriers, varying age of colonoscopy initiation (5-year increments from 25-40 years), and surveillance intervals (1-5 years). We assessed the optimal strategy for each gene, defined as the strategy with the highest quality-adjusted life-years and incremental cost-effectiveness ratio below a $100,000 willingness-to-pay threshold.
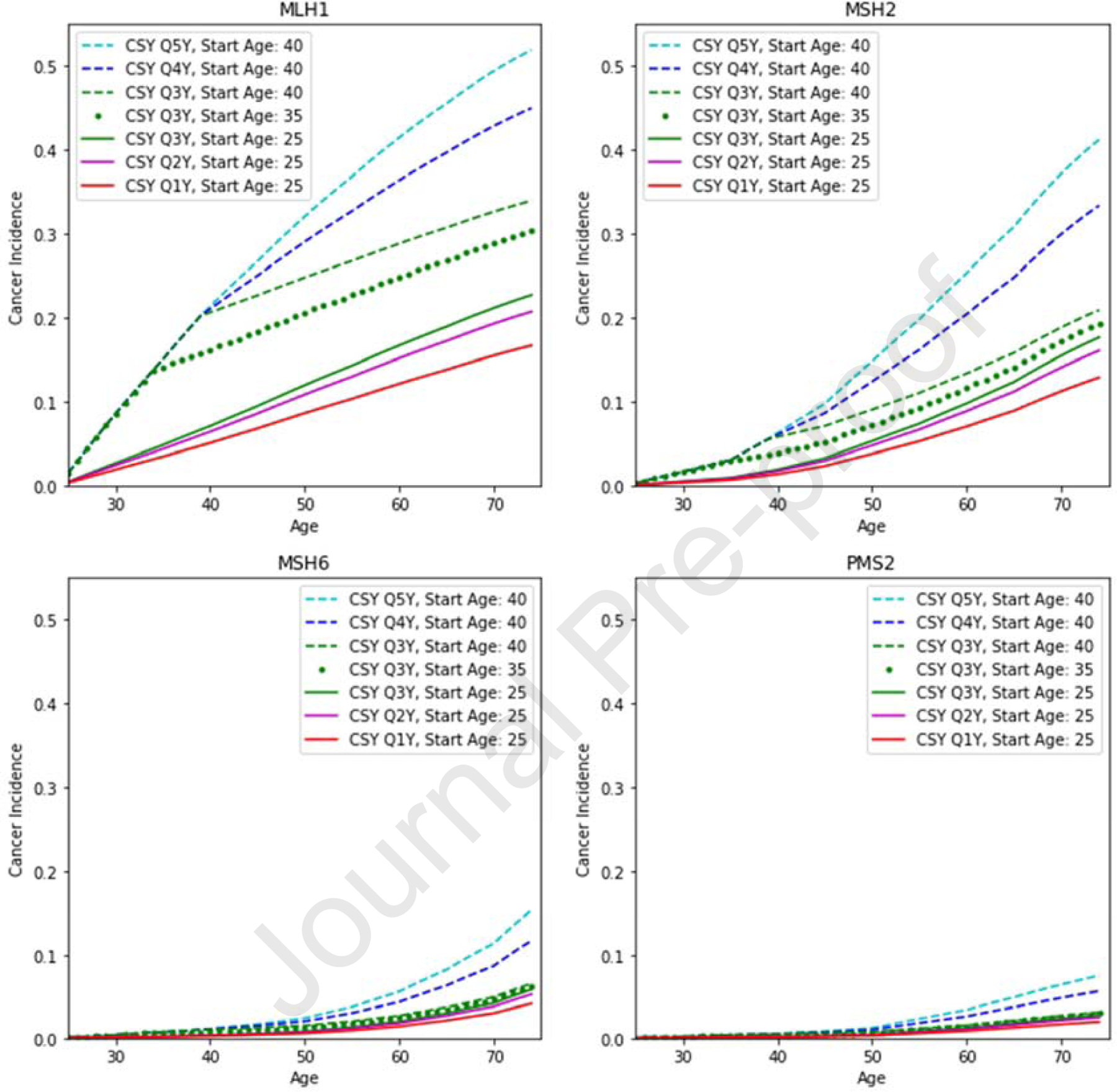
Results: Optimal surveillance for patients with pathogenic variants in the MLH1 and MSH2 genes was colonoscopy starting at age 25 years, with 1- to 2-year surveillance intervals. Initiating colonoscopy at age 35 and 40 years, with 3-year intervals, was cost-effective for patients with pathogenic variants in MSH6 or PMS2, respectively.
Conclusions: We developed a simulation model to select optimal surveillance starting ages and intervals for patients with Lynch syndrome based on MMR variant. The model supports recommendations for intensive surveillance of patients with Lynch syndrome-associated variants in MLH1 or MSH2. However, for patients with Lynch syndrome-associated variants of MSH6 or PMS2, later initiation of surveillance at 35 and 40 years, respectively, and at 3-year intervals, can be considered.
Keywords: Colorectal Cancer; Cost-Effectiveness; Genetic Cancer Syndromes; Surveillance.
Copyright © 2021 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosures:
No relevant financial, professional, or personal conflicts to disclose.
Figures
Comment in
-
Tailoring Colorectal Cancer Surveillance in Lynch Syndrome: More Is Not Always Better.Gastroenterology. 2021 Aug;161(2):411-412. doi: 10.1053/j.gastro.2021.04.069. Epub 2021 May 5. Gastroenterology. 2021. PMID: 33961883 No abstract available.
References
-
- Maxwell KN, Domchek SM, Nathanson KL, Robson ME. Population frequency of germline BRCA1/2 mutations. J Clin Oncol 2016; 34(34):4183. - PubMed
-
- Järvinen HJ, Aarnio M, Mustonen H, et al. Controlled 15-year trial on screening for colorectal cancer in families with hereditary nonpolyposis colorectal cancer. Gastroenterology 2000; 118(5):829–834. - PubMed
-
- Vasen HF, Abdirahman M, Brohet R, et al. One to 2-year surveillance intervals reduce risk of colorectal cancer in families with Lynch syndrome. Gastroenterology 2010; 138(7):2300–6. - PubMed
-
- Mecklin J-P, Aarnio M, Läärä E, et al. Development of colorectal tumors in colonoscopic surveillance in Lynch syndrome. Gastroenterology 2007; 133(4):1093–1098. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
