

Intensity-modulated proton therapy for oropharyngeal cancer reduces rates of late xerostomia
- PMID: 33839202
- PMCID: PMC8349568
- DOI: 10.1016/j.radonc.2021.03.036
Intensity-modulated proton therapy for oropharyngeal cancer reduces rates of late xerostomia
Abstract
Background and purpose: To determine rates of xerostomia after intensity-modulated radiotherapy (IMRT) or intensity-modulated proton therapy (IMPT) for oropharyngeal cancer (OPC) and identify dosimetric factors associated with xerostomia risk.
Materials and methods: Patients with OPC who received IMRT (n = 429) or IMPT (n = 103) from January 2011 through June 2015 at a single institution were studied retrospectively. Every 3 months after treatment, each patient completed an eight-item self-reported xerostomia-specific questionnaire (XQ; summary XQ score, 0-100). An XQ score of 50 was selected as the demarcation value for moderate-severe (XQs ≥ 50) and no-mild (XQs < 50) xerostomia. The mean doses and percent volumes of organs at risk receiving various doses (V5-V70) were extracted from the initial treatment plans. The dosimetric variables and xerostomia risk were compared using an independent-sample t-test or chi-square test.
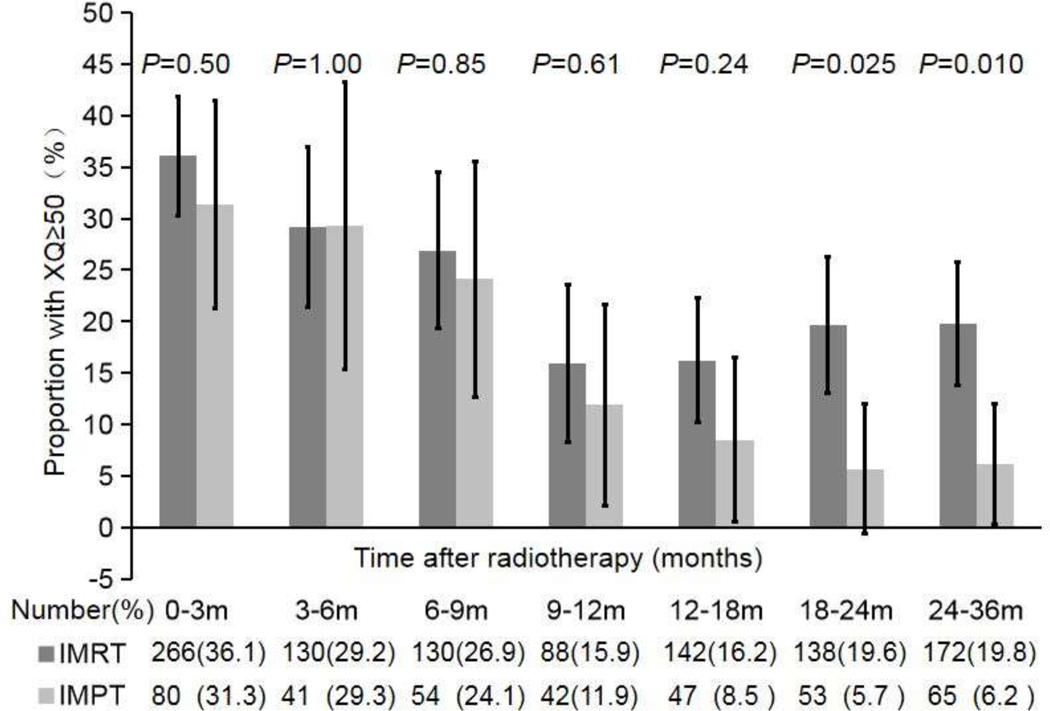
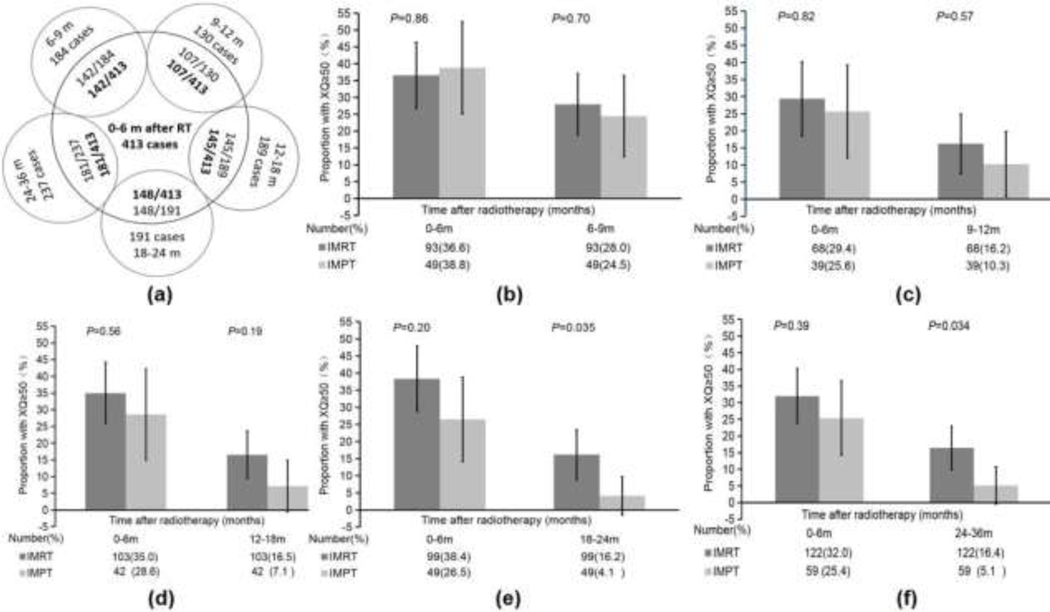
Results: The median follow-up time was 36.2 months. The proportions of patients with moderate-severe xerostomia were similar in the two treatment groups up to 18 months after treatment. However, moderate-severe xerostomia was less common in the IMPT group than in the IMRT group at 18-24 months (6% vs. 20%; p = 0.025) and 24-36 months (6% vs. 20%; p = 0.01). During the late xerostomia period (24-36 months), high dose/volume exposures (V25-V70) in the oral cavity were associated with high proportions of patients with moderate-severe xerostomia (all p < 0.05), but dosimetric variables regarding the salivary glands were not associated with late xerostomia.
Conclusion: IMPT was associated with less late xerostomia than was IMRT in OPC patients. Oral cavity dosimetric variables were related to the occurrence of late xerostomia.
Keywords: Intensity-modulated proton therapy; Intensity-modulated radiotherapy; Oropharyngeal cancer; Xerostomia.
Copyright © 2021 Elsevier B.V. All rights reserved.
Conflict of interest statement
Conflict of interest statement: The authors declare no conflicts of interest.
Figures
References
-
- Clavel S, Nguyen DH, Fortin B, Després P, Khaouam N, Donath D, et al. Simultaneous integrated boost using intensity-modulated radiotherapy compared with conventional radiotherapy in patients treated with concurrent carboplatin and 5-fluorouracil for locally advanced oropharyngeal carcinoma. Int J Radiat Oncol Biol Phys. 2012;82:582–9. - PubMed
-
- Lee NY, de Arruda FF, Puri DR, Wolden SL, Narayana A, Mechalakos J, et al. A comparison of intensity-modulated radiation therapy and concomitant boost radiotherapy in the setting of concurrent chemotherapy for locally advanced oropharyngeal carcinoma. Int J Radiat Oncol Biol Phys. 2006;66:966–74. - PubMed
-
- Eisbruch A, Rhodus N, Rosenthal D, Murphy B, Rasch C, Sonis S, et al. How should we measure and report radiotherapy-induced xerostomia? Semin Radiat Oncol. 2003;13:226–34. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
