

Hepatocellular carcinoma progression during bridging before liver transplantation
- PMID: 33839747
- PMCID: PMC8038254
- DOI: 10.1093/bjsopen/zrab005
Hepatocellular carcinoma progression during bridging before liver transplantation
Abstract
Background: Recipient selection for liver transplantation in hepatocellular carcinoma (HCC) is based primarily on criteria affecting the chance of long-term success. Here, the relationship between pretransplant bridging therapy and long-term survival was investigated in a subgroup analysis of the SiLVER Study.
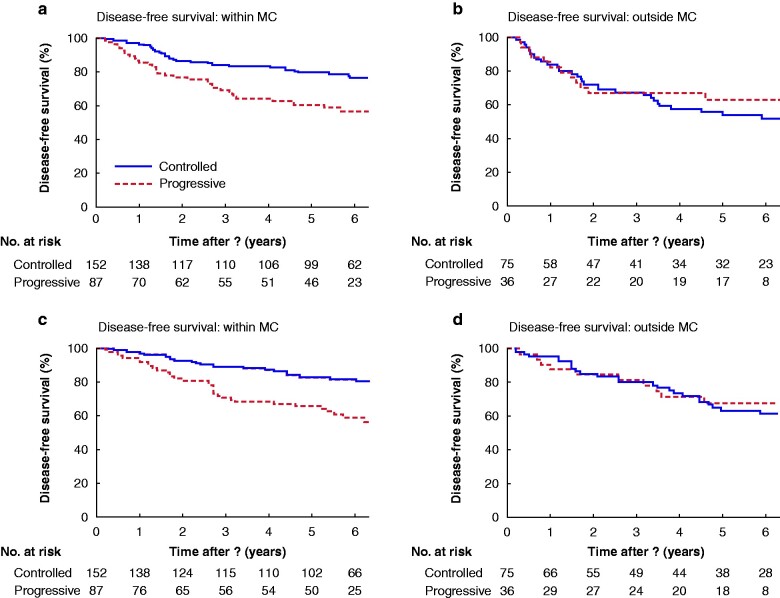
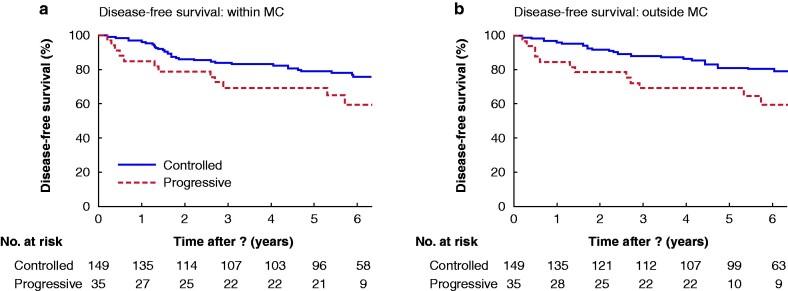
Methods: Response to bridging, as defined by comparison of imaging at the time of listing and post-transplant pathology report, was categorized into controlled versus progressive disease (more than 20 per cent tumour growth or development of new lesions).
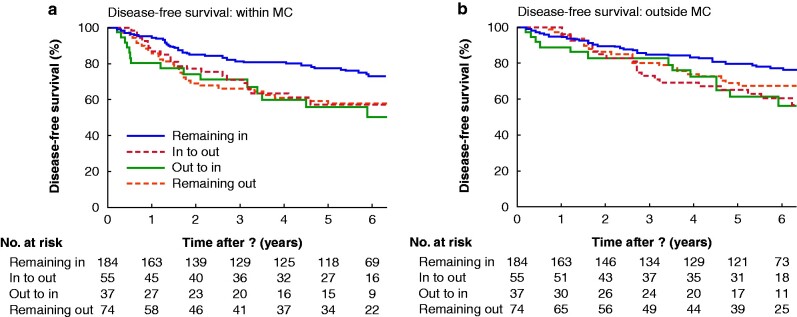
Results: Of 525 patients with HCC who had liver transplantation, 350 recipients underwent pretransplant bridging therapy. Tumour progression despite bridging was an independent risk factor affecting overall survival (hazard ratio 1.80; P = 0.005). For patients within the Milan criteria (MC) at listing, mean overall survival was longer for those with controlled versus progressive disease (6.8 versus 5.8 years; P < 0.001). Importantly, patients with HCCs outside the MC that were downsized to within the MC before liver transplantation had poor outcomes compared with patients who never exceeded the MC (mean overall survival 6.2 versus 6.6 years respectively; P = 0.030).
Conclusion: Patients with HCCs within the MC that did not show tumour progression under locoregional therapy had the best outcomes after liver transplantation. Downstaging into the limits of the MC did not improve the probability of survival.Prognostic factors determining the long-term success of liver transplantation in patients with hepatocellular carcinoma are still under discussion. A subgroup analysis of the SiLVER trial showed that disease control under bridging therapy is strongly associated with improved prognosis in terms of overall survival. However, in tumours exceeding the limits of the Milan criteria, downstaging did not restore the probability of survival compared with that of patients within the Milan criteria.
© The Author(s) 2021. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures
References
-
- Llovet JM, Montal R, Sia D, Finn RS. Molecular therapies and precision medicine for hepatocellular carcinoma. Nat Rev Clin Oncol 2018;15:599–616 - PubMed
-
- Llovet JM, Bru C, Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Dis 1999;19:329–338 - PubMed
-
- Sapisochin G, Bruix J. Liver transplantation for hepatocellular carcinoma: outcomes and novel surgical approaches. Nat Rev Gastroenterol Hepatol 2017;14:203–217 - PubMed
-
- Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med 1996;334:693–699 - PubMed
-
- Mazzaferro V, Bhoori S, Sposito C, Bongini M, Langer M, Miceli R et al. Milan criteria in liver transplantation for hepatocellular carcinoma: an evidence-based analysis of 15 years of experience. Liver Transpl 2011;17:S44–S57 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
