

Relative Predictive Value of Circulating Immune Markers in US Adults Without Cardiovascular Disease: Implications for Risk Reclassification
- PMID: 33840521
- PMCID: PMC8683138
- DOI: 10.1016/j.mayocp.2020.11.027
Relative Predictive Value of Circulating Immune Markers in US Adults Without Cardiovascular Disease: Implications for Risk Reclassification
Abstract
Objective: To investigate the relative predictive value of circulating immune cell markers for cardiovascular mortality in ambulatory adults without cardiovascular disease.
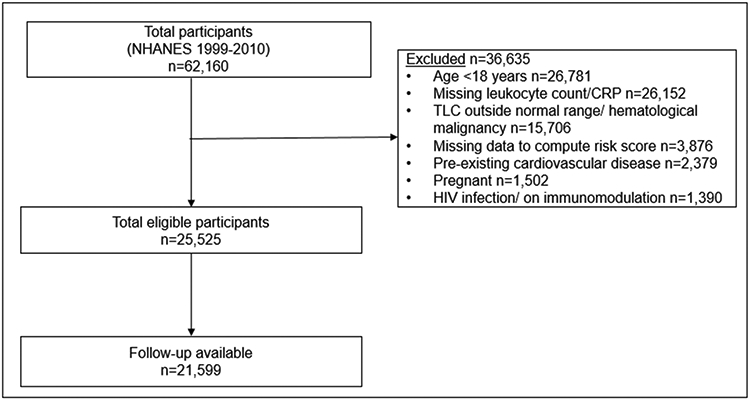
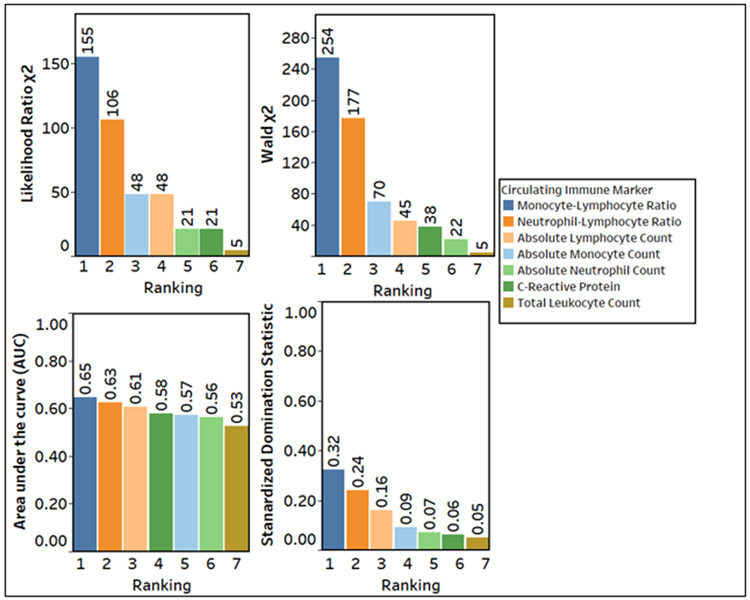
Methods: We analyzed data of participants enrolled in the National Health and Nutrition Examination Survey from January 1, 1999, to December 31, 2010, with the total leukocyte count within a normal range (4000-11,000 cells/μL [to convert to cells ×109/L, multiply by 0.001]) and without cardiovascular disease. The relative predictive value of circulating immune cell markers measured at enrollment-including total leukocyte count, absolute neutrophil count, absolute lymphocyte count, absolute monocyte count, monocyte-lymphocyte ratio (MLR), neutrophil-lymphocyte ratio, and C-reactive protein-for cardiovascular mortality was evaluated. The marker with the best predictive value was added to the 10-year atherosclerotic cardiovascular disease (ASCVD) risk score to estimate net risk reclassification indices for 10-year cardiovascular mortality.
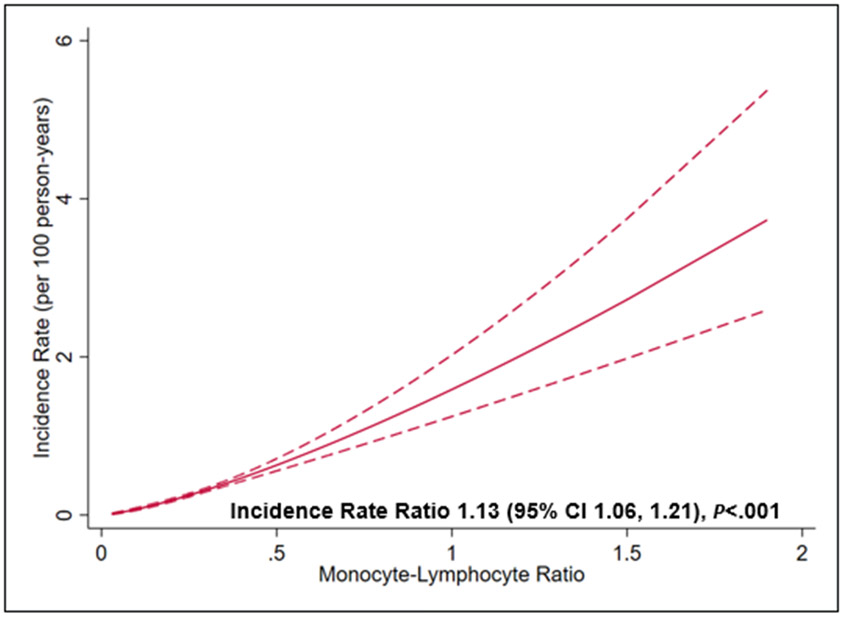
Results: Among 21,599 participants eligible for this analysis, the median age was 47 years (interquartile range, 34-63 years); 10,651 (49.2%) participants were women, and 10,713 (49.5%) were self-reported non-Hispanic white. During a median follow-up of 9.6 years (interquartile range, 6.8-13.1 years), there were 627 cardiovascular deaths. MLR had the best predictive value for cardiovascular mortality. The addition of elevated MLR (≥0.3) to the 10-year ASCVD risk score improved the classification by 2.7%±1.4% (P=.04). Elevated MLR had better predictive value than C-reactive protein and several components of the 10-year ASCVD risk score.
Conclusion: Among ambulatory US adults without preexisting cardiovascular disease, we found that MLR had the best predictive value for cardiovascular mortality among circulating immune markers. The addition of MLR to the 10-year risk score significantly improved the risk classification of participants.
Published by Elsevier Inc.
Conflict of interest statement
Figures

Similar articles
-
Elevated neutrophil-to-lymphocyte and monocyte-to-lymphocyte ratios are associated with increased flares and elevated cardiovascular disease risk in gout.Scand J Rheumatol. 2025 Mar;54(2):142-146. doi: 10.1080/03009742.2024.2421622. Epub 2025 Jan 17. Scand J Rheumatol. 2025. PMID: 39819380
-
Assessment efficacy of neutrophil-lymphocyte ratio and monocyte-lymphocyte ratio in preeclampsia.J Reprod Immunol. 2019 Apr;132:29-34. doi: 10.1016/j.jri.2019.02.001. Epub 2019 Mar 6. J Reprod Immunol. 2019. PMID: 30861482
-
Which leukocyte subsets predict cardiovascular mortality? From the LUdwigshafen RIsk and Cardiovascular Health (LURIC) Study.Atherosclerosis. 2012 Sep;224(1):161-9. doi: 10.1016/j.atherosclerosis.2012.04.012. Epub 2012 Jun 9. Atherosclerosis. 2012. PMID: 22809446
-
Low lymphocyte count and high monocyte count predicts poor prognosis of gastric cancer.BMC Gastroenterol. 2018 Oct 11;18(1):148. doi: 10.1186/s12876-018-0877-9. BMC Gastroenterol. 2018. PMID: 30305076 Free PMC article. Review.
-
Assessing the role of circulating, genetic, and imaging biomarkers in cardiovascular risk prediction.Circulation. 2011 Feb 8;123(5):551-65. doi: 10.1161/CIRCULATIONAHA.109.912568. Circulation. 2011. PMID: 21300963 Free PMC article. Review. No abstract available.
Cited by
-
Development of a prediction model to estimate the 5-year risk of cardiovascular events and all-cause mortality in haemodialysis patients: a retrospective study.PeerJ. 2022 Nov 9;10:e14316. doi: 10.7717/peerj.14316. eCollection 2022. PeerJ. 2022. PMID: 36389426 Free PMC article.
-
The Absolute Monocyte Count at Diagnosis Affects Prognosis in Myelodysplastic Syndromes Independently of the IPSS-R Risk Score.Cancers (Basel). 2023 Jul 11;15(14):3572. doi: 10.3390/cancers15143572. Cancers (Basel). 2023. PMID: 37509235 Free PMC article.
-
Inflammatory Hematological Indices, Cardiovascular Disease and Mortality: A Narrative Review.Arq Bras Cardiol. 2024 Aug 26;121(7):e20230752. doi: 10.36660/abc.20230752. eCollection 2024. Arq Bras Cardiol. 2024. PMID: 39193999 Free PMC article. Review. English, Portuguese.
-
Associations of lifestyle characteristics with circulating immune markers in the general population based on NHANES 1999 to 2014.Sci Rep. 2024 Jun 11;14(1):13444. doi: 10.1038/s41598-024-63875-2. Sci Rep. 2024. PMID: 38862546 Free PMC article.
-
Monocyte-lymphocyte ratio predicts cardiovascular diseases death in individuals with type 2 diabetes.J Diabetes Investig. 2025 Jan;16(1):137-145. doi: 10.1111/jdi.14329. Epub 2024 Nov 6. J Diabetes Investig. 2025. PMID: 39503178 Free PMC article.
References
-
- Friedman GD, Klatsky AL, Siegelaub AB. The Leukocyte Count as a Predictor of Myocardial Infarction. New England Journal of Medicine. 1974;290(23):1275–1278. - PubMed
-
- Ernst E, Hammerschmidt DE, Bagge U, Matrai A, Dormandy JA. Leukocytes and the risk of ischemic diseases. Jama. 1987;257(17):2318–2324. - PubMed
-
- Sweetnam PM, Thomas HF, Yarnell JW, Baker IA, Elwood PC. Total and differential leukocyte counts as predictors of ischemic heart disease: the Caerphilly and Speedwell studies. American journal of epidemiology. 1997;145(5):416–421. - PubMed
-
- D'Agostino RB Sr., Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008;117(6):743–753. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
