

Mortality after bleeding versus myocardial infarction in coronary artery disease: a systematic review and meta-analysis
- PMID: 33840639
- PMCID: PMC9725060
- DOI: 10.4244/EIJ-D-20-01197
Mortality after bleeding versus myocardial infarction in coronary artery disease: a systematic review and meta-analysis
Abstract
Background: Bleeding is the principal safety concern of antithrombotic therapy and occurs frequently among patients with coronary artery disease (CAD).
Aims: We aimed to evaluate the prognostic impact of bleeding on mortality compared with that of myocardial infarction (MI) in patients with CAD.
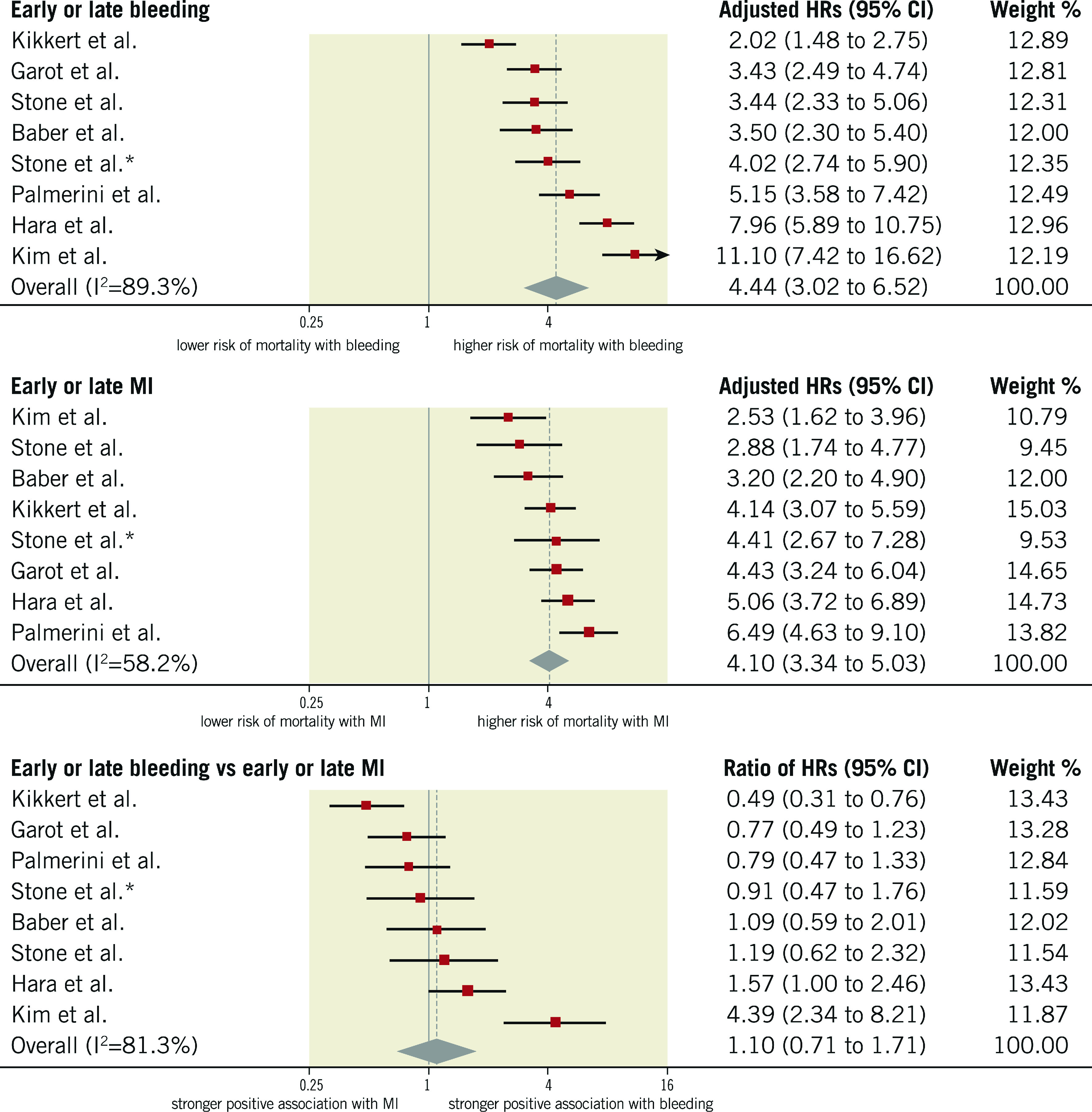
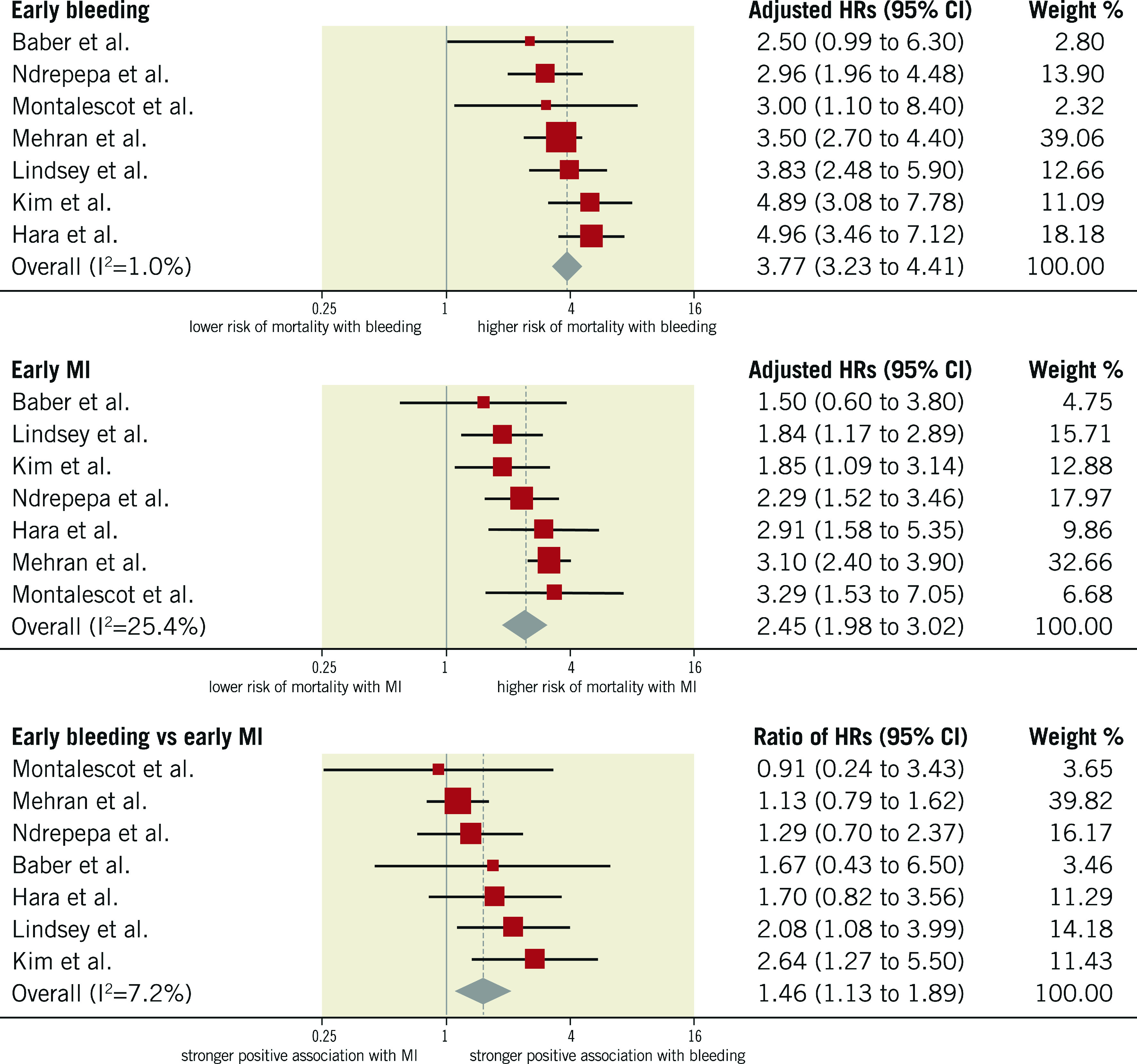
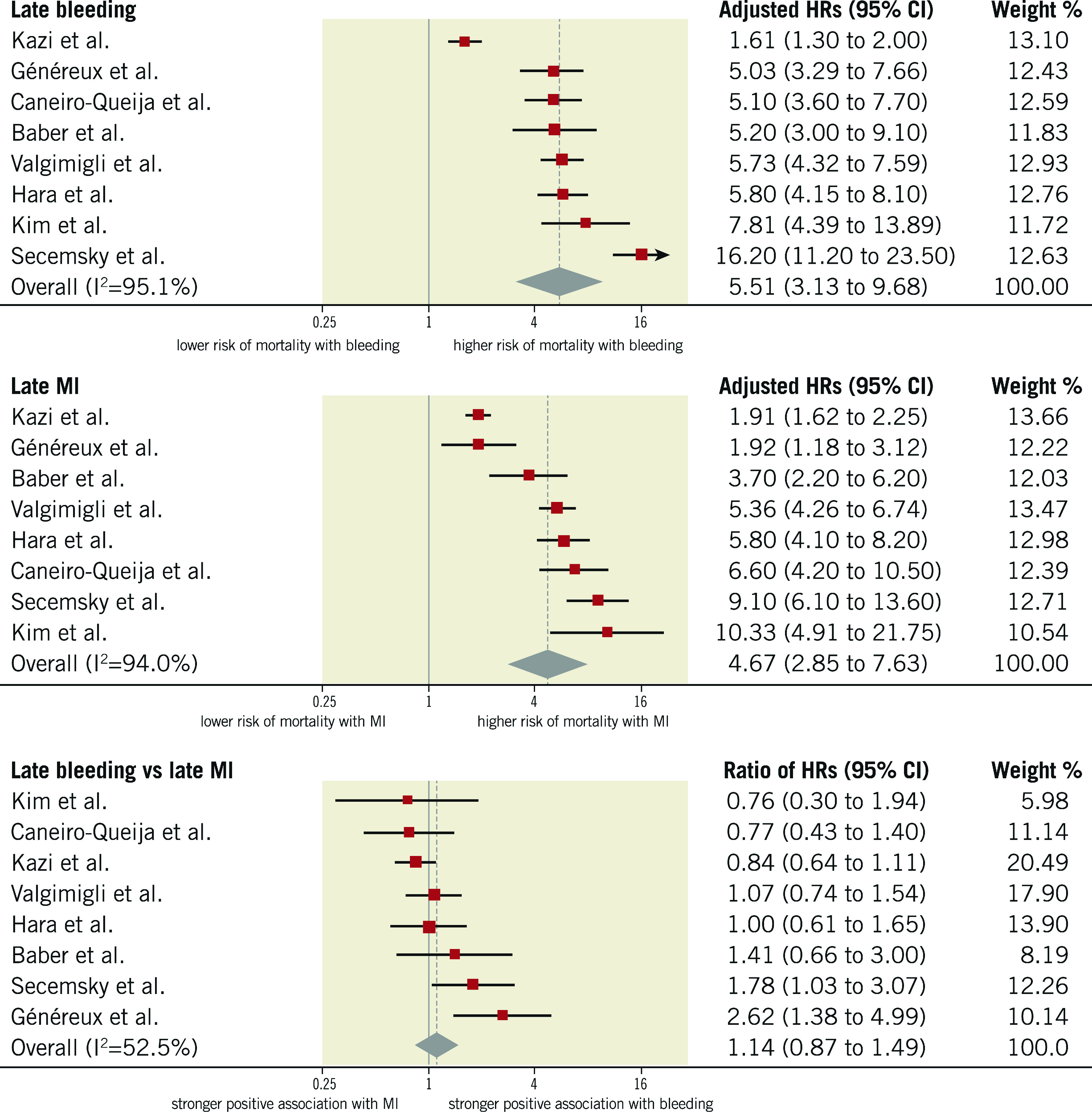
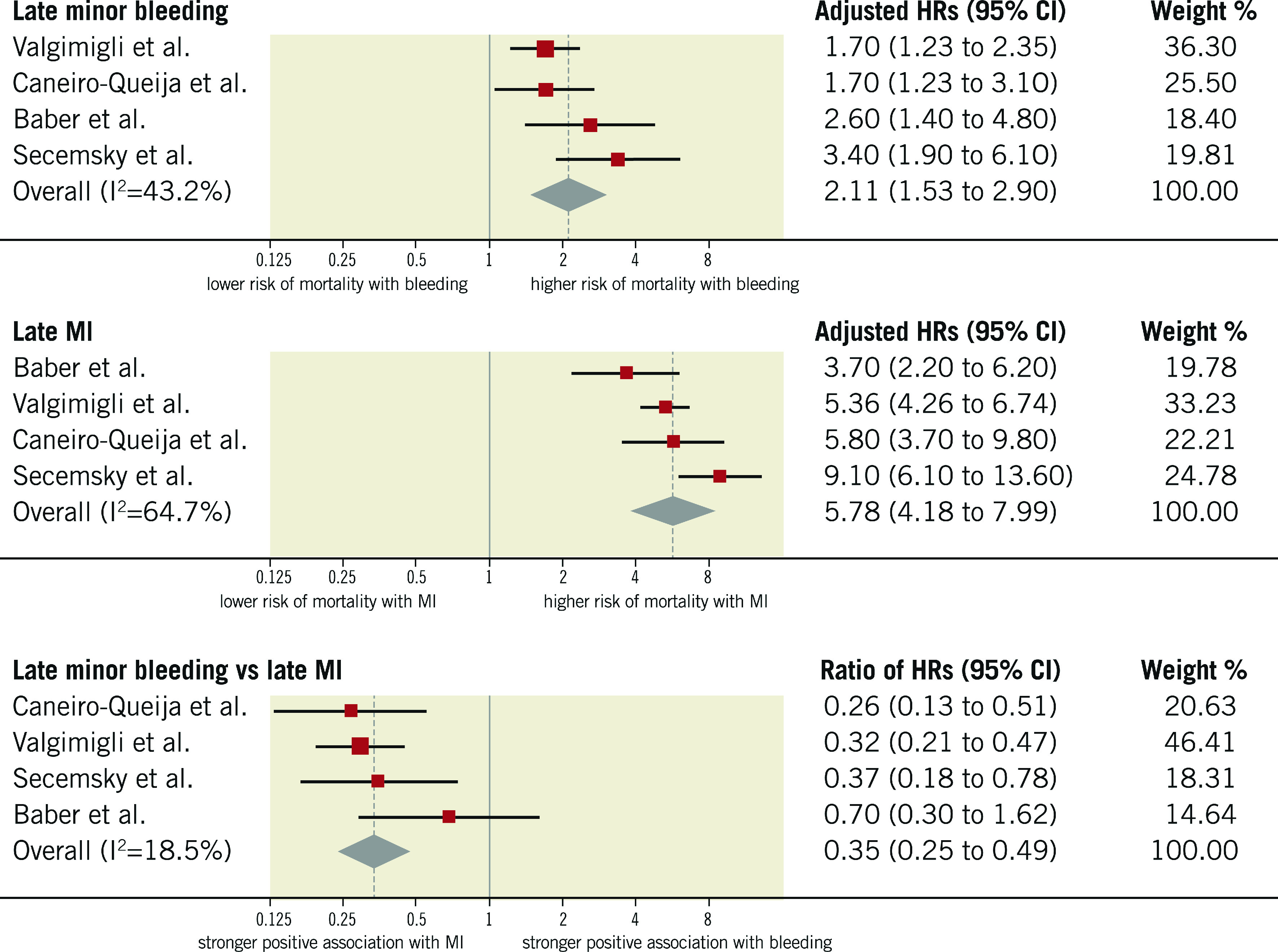
Methods: We searched Medline and Embase for studies that included patients with CAD and that reported both the association between the occurrence of bleeding and mortality, and between the occurrence of MI and mortality within the same population. Adjusted hazard ratios (HRs) for mortality associated with bleeding and MI were extracted and ratios of hazard ratios (rHRs) were pooled by using inverse variance weighted random effects meta-analyses. Early events included periprocedural or within 30-day events after revascularisation or acute coronary syndrome (ACS). Late events included spontaneous or beyond 30-day events after revascularisation or ACS.
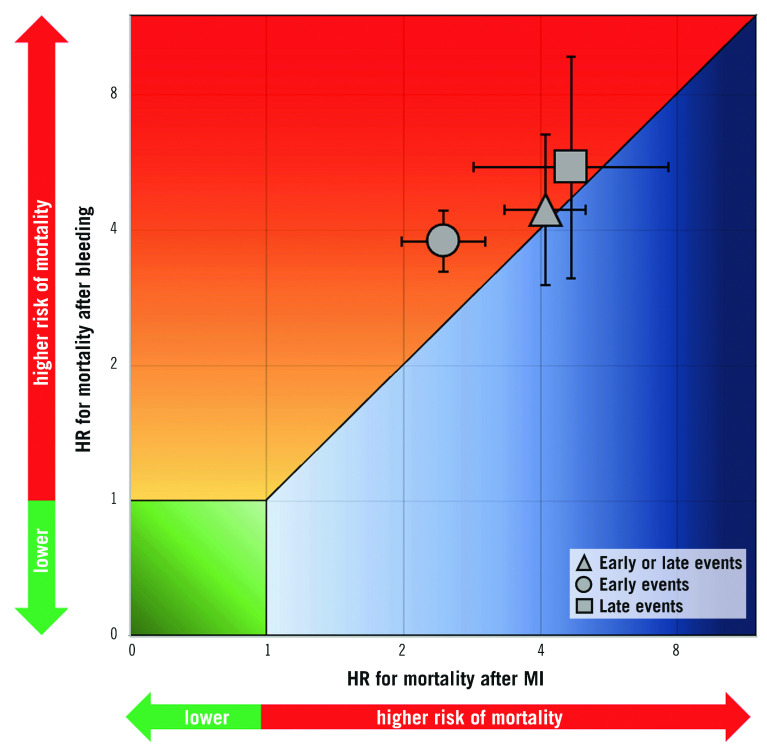
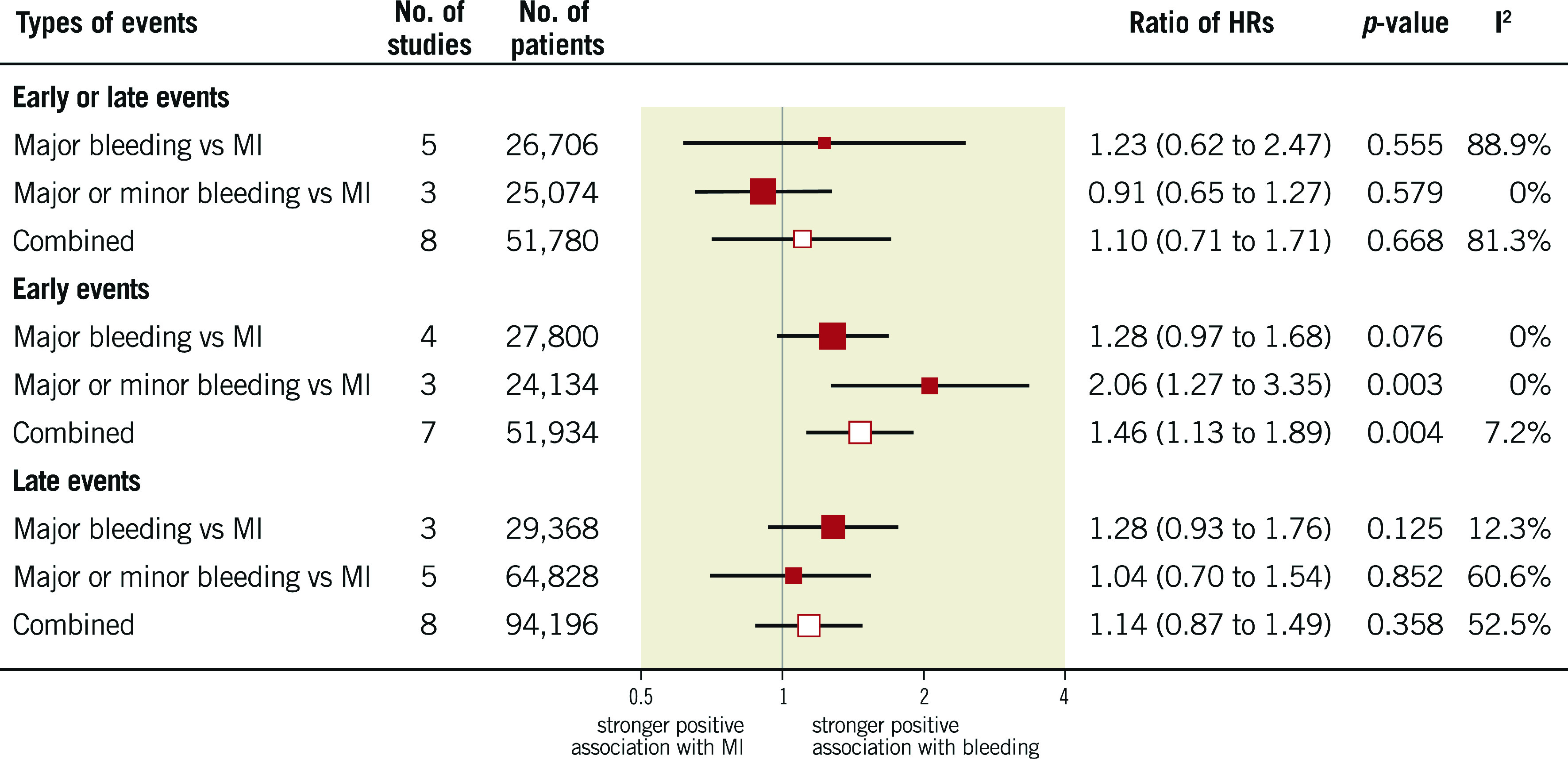
Results: A total of 141,059 patients were included across 16 studies; 128,660 (91%) underwent percutaneous coronary intervention. Major bleeding increased the risk of mortality to the same extent as MI (rHRsbleedingvsMI 1.10, 95% CI: 0.71-1.71, p=0.668). Early bleeding was associated with a higher risk of mortality than early MI (rHRsbleedingvsMI 1.46, 95% CI: 1.13-1.89, p=0.004), although this finding was not present when only randomised trials were included. Late bleeding was prognostically comparable to late MI (rHRsbleedingvsMI 1.14, 95% CI: 0.87-1.49, p=0.358).
Conclusions: Compared with MI, major and late bleeding is associated with a similar increase in mortality, whereas early bleeding might have a stronger association with mortality.
Conflict of interest statement
R. Piccolo reports personal fees from Abbott Vascular. S. Windecker reports research and educational grants to the institution from Abbott, Amgen, BMS, Bayer, Boston Scientific, Biotronik, Cardinal Health, CSL Behring, Daiichi Sankyo, Edwards Lifesciences, Johnson&Johnson, Medtronic, Querbet, Polares, Sanofi, Terumo, and Sinomed. M. Valgimigli reports grants and personal fees from Terumo, personal fees from AstraZeneca, Alvimedica/CID, Abbott Vascular, Daiichi Sankyo, Opsens, Bayer, CoreFlow, Idorsia Pharmaceuticals Ltd, Universität Basel Dept. Klinische Forschung, Vifor, Bristol Myers Squibb SA, iVascular, and Medscape. P. Jüni serves as unpaid member of the steering group of trials funded by AstraZeneca, Biotronik, Biosensors, St. Jude Medical and The Medicines Company, has received research grants to the institution from AstraZeneca, Biotronik, Biosensors International, Eli Lilly and The Medicines Company, and honoraria to the institution for participation in advisory boards and/or consulting from Amgen, Ava and Fresenius, but has not received personal payments by any pharmaceutical company or device manufacturer, and he has no other relationships or activities that could appear to have influenced the submitted work. The other authors have no conflicts of interest to declare.
Figures
Comment in
-
Walking the tightrope between ischaemia and bleeding.EuroIntervention. 2021 Sep 20;17(7):527-529. doi: 10.4244/EIJV17I7A93. EuroIntervention. 2021. PMID: 34554092 Free PMC article. No abstract available.
References
-
- Mauri L, Kereiakes DJ, Yeh RW, Driscoll-Shempp P, Cutlip DE, Steg PG, Normand SL, Braunwald E, Wiviott SD, Cohen DJ, Holmes DR, Jr, Krucoff MW, Hermiller J, Dauerman HL, Simon DI, Kandzari DE, Garratt KN, Lee DP, Pow TK, Ver Lee P, Rinaldi MJ, Massaro JM DAPT Study Investigators. Twelve or 30 months of dual-antiplatelet therapy after drug-eluting stents. N Engl J Med. 2014;371:2155–66. - PMC - PubMed
-
- Bonaca MP, Bhatt DL, Cohen M, Steg PG, Storey RF, Jensen EC, Magnani G, Bansilal S, Fish MP, Im K, Bengtsson O, Oude Ophuis T, Budaj A, Theroux P, Ruda M, Hamm C, Goto S, Spinar J, Nicolau JC, Kiss RG, Murphy SA, Wiviott SD, Held P, Braunwald E, Sabatine MS PEGASUS-TIMI 54 Steering Committee and Investigators. Long-term use of ticagrelor in patients with prior myocardial infarction. N Engl J Med. 2015;372:1791–800. - PubMed
-
- Spertus JA, Decker C, Gialde E, Jones PG, McNulty EJ, Bach R, Chhatriwalla AK. Precision medicine to improve use of bleeding avoidance strategies and reduce bleeding in patients undergoing percutaneous coronary intervention: prospective cohort study before and after implementation of personalized bleeding risks. BMJ. 2015;350:1302. doi: 10.1136/bmj.h1302. - DOI - PMC - PubMed
-
- Urban P, Mehran R, Colleran R, Angiolillo DJ, Byrne RA, Capodanno D, Cuisset T, Cutlip D, Eerdmans P, Eikelboom J, Farb A, Gibson CM, Gregson J, Haude M, James SK, Kim HS, Kimura T, Konishi A, Laschinger J, Leon MB, Magee PFA, Mitsutake Y, Mylotte D, Pocock S, Price MJ, Rao SV, Spitzer E, Stockbridge N, Valgimigli M, Varenne O, Windhoevel U, Yeh RW, Krucoff MW, Morice MC. Defining High Bleeding Risk in Patients Undergoing Percutaneous Coronary Intervention. Circulation. 2019;140:240–61. doi: 10.1161/CIRCULATIONAHA.119.040167. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous