

Thrombotic microangiopathies assessment: mind the complement
- PMID: 33841853
- PMCID: PMC8023218
- DOI: 10.1093/ckj/sfaa195
Thrombotic microangiopathies assessment: mind the complement
Abstract
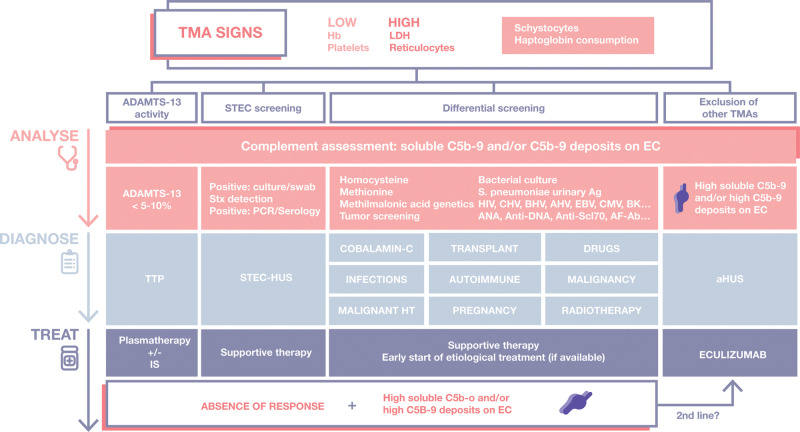
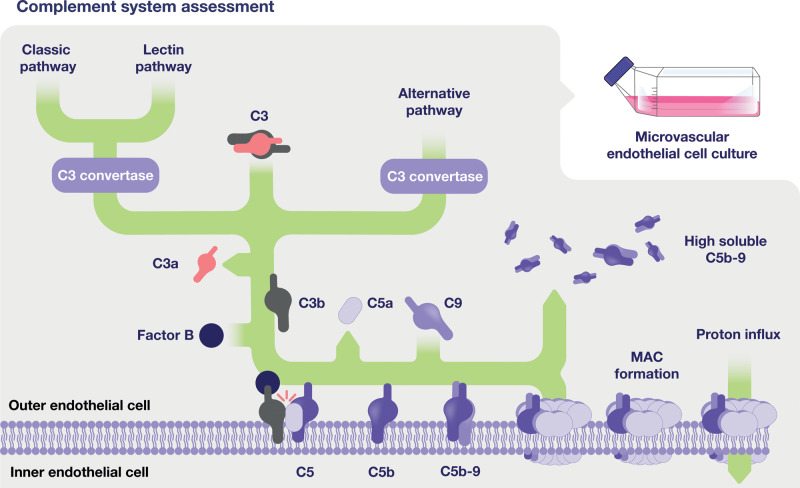
When faced with microangiopathic haemolytic anaemia, thrombocytopenia and organ dysfunction, clinicians should suspect thrombotic microangiopathy (TMA). The endothelial damage that leads to this histological lesion can be triggered by several conditions or diseases, hindering an early diagnosis and aetiological treatment. However, due to systemic involvement in TMA and its low incidence, an accurate early diagnosis is often troublesome. In the last few decades, major improvements have been made in the pathophysiological knowledge of TMAs such as thrombotic thrombocytopenic purpura [TTP, caused by ADAMTS-13 (a disintegrin and metalloproteinase with a thrombospondin Type 1 motif, member 13) deficiency] and atypical haemolytic uraemic syndrome (aHUS, associated with dysregulation of the alternative complement pathway), together with enhancements in patient management due to new diagnostic tools and treatments. However, diagnosis of aHUS requires the exclusion of all the other entities that can cause TMA, delaying the introduction of terminal complement blockers, which have shown high efficacy in haemolysis control and especially in avoiding organ damage if used early. Importantly, there is increasing evidence that other forms of TMA could present overactivation of the complement system, worsening their clinical progression. This review addresses the diagnostic and therapeutic approach when there is clinical suspicion of TMA, emphasizing complement evaluation as a potential tool for the inclusive diagnosis of aHUS, as well as for the improvement of current knowledge of its pathophysiological involvement in other TMAs. The development of both new complement activation biomarkers and inhibitory treatments will probably improve the management of TMA patients in the near future, reducing response times and improving patient outcomes.
Keywords: C5b-9 deposits; complement system; endothelial cells (ECs); membrane attack complex (C5b-9); soluble C5b-9; thrombotic microangiopathies.
© The Author(s) 2020. Published by Oxford University Press on behalf of ERA-EDTA.
Figures


References
-
- Campistol JM, Arias M, Ariceta G. et al. An update for atypical haemolytic uraemic syndrome: diagnosis and treatment. A consensus document. Nefrologia 2015; 35: 421–447 - PubMed
-
- George JN, Nester CM.. Syndromes of thrombotic microangiopathy. N Engl J Med 2014; 371: 654–666 - PubMed
-
- Shatzel JJ, Taylor JA.. Syndromes of thrombotic microangiopathy. Med Clin North Am 2017; 101: 395–415 - PubMed
-
- Noris M, Mescia F, Remuzzi G.. STEC-HUS, atypical HUS and TTP are all diseases of complement activation. Nat Rev Nephrol 2012; 8: 622–633 - PubMed
