

Minimally invasive aortic valve surgery
- PMID: 33841981
- PMCID: PMC8024826
- DOI: 10.21037/jtd-20-1968
Minimally invasive aortic valve surgery
Abstract
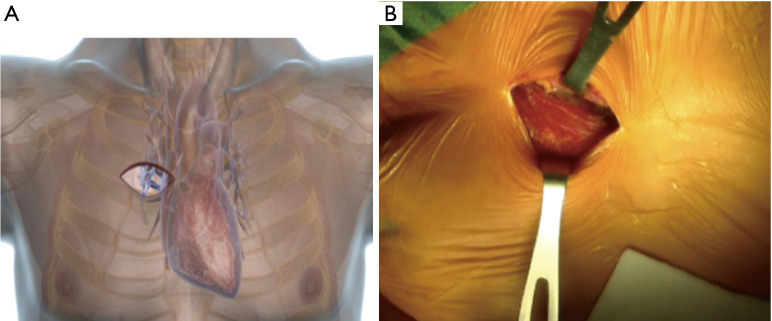
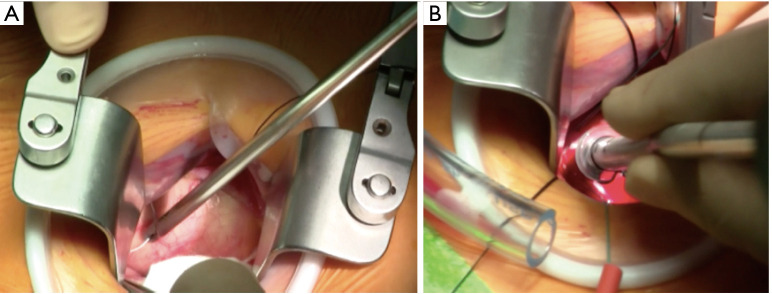
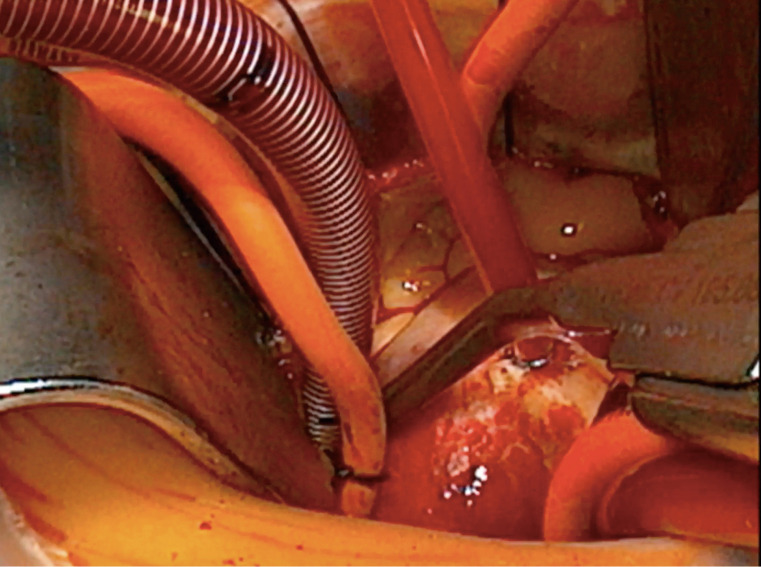
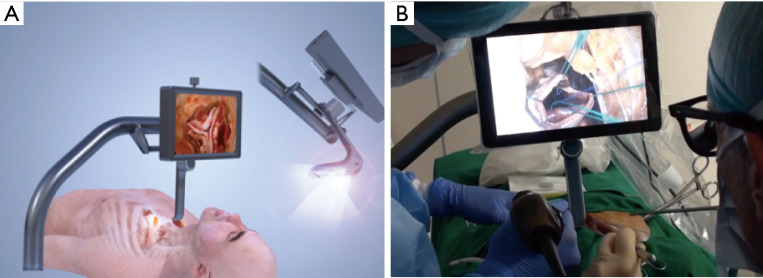
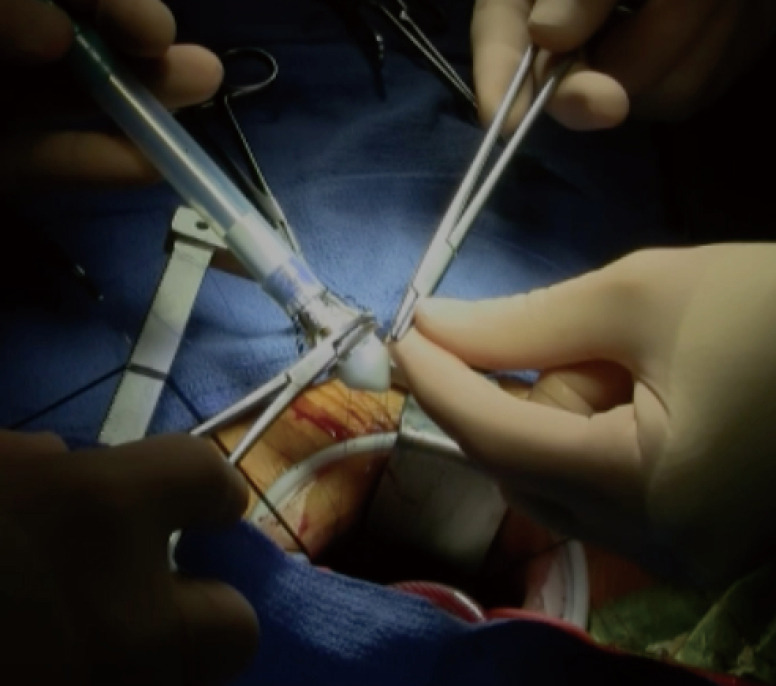
Since their introduction, it has been demonstrated that minimally invasive aortic valve replacement (MIAVR) approaches are safe and effective for the treatment of aortic valve diseases. To date, the main advantage of these approaches is represented by the reduced surgical trauma, with a subsequent reduced complication rate and faster recovery. This makes such approaches an appealing choice also for frail patients [obese, aged, chronic obstructive pulmonary disease (COPD)]. The standardization of the minimally invasive techniques, together with the implementation of preoperative workup and anesthesiological intra- and post-operative care, led to an amelioration of surgical results and reduction of surgical times. Moreover, the improvement of surgical technology and the introduction of new devices such as sutureless and rapid deployment (SURD) valves, has helped the achievement of comparable results to traditional surgery. However, transcatheter technologies are nowadays more and more important in the treatment of aortic valve disease, also in low risk patients. For this reason surgeons should put new efforts for further reducing the surgical trauma in the future, even taking inspiration from other disciplines. In this review, we aim to present a review of literature evidences regarding minimally invasive treatment of aortic diseases, also reflecting our personal experience with MIAVR techniques. This review could represent a tool for a well-structured patient assessment and preoperative planning, in order to safely carrying out an MIAVR procedure with satisfactory outcomes.
Keywords: Minimally invasive; aortic valve surgery; minimally invasive cardiac surgery aortic valve replacement (MICS AVR); ministernotomy (MS); right anterior thoracotomy (RAT).
2021 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/jtd-20-1968). The series “Minimally Invasive Cardiac Surgery” was commissioned by the editorial office without any funding or sponsorship. AM serves as an unpaid editorial board member of Journal of Thoracic Disease from Feb 2021 to Jan 2023. Dr. AM and Dr. MG report personal fees from LivaNova, outside the submitted work. The authors have no other conflicts of interest to declare.
Figures
References
-
- STS National Database Spring 2003, Executive summary, Duke Clinical Research Institute, Durham, NC; 2003.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources