

Morphea: progress to date and the road ahead
- PMID: 33842658
- PMCID: PMC8033330
- DOI: 10.21037/atm-20-6222
Morphea: progress to date and the road ahead
Abstract
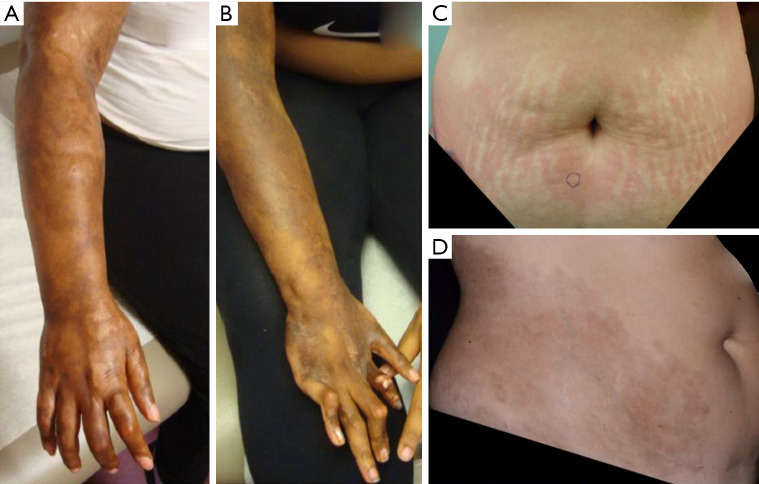
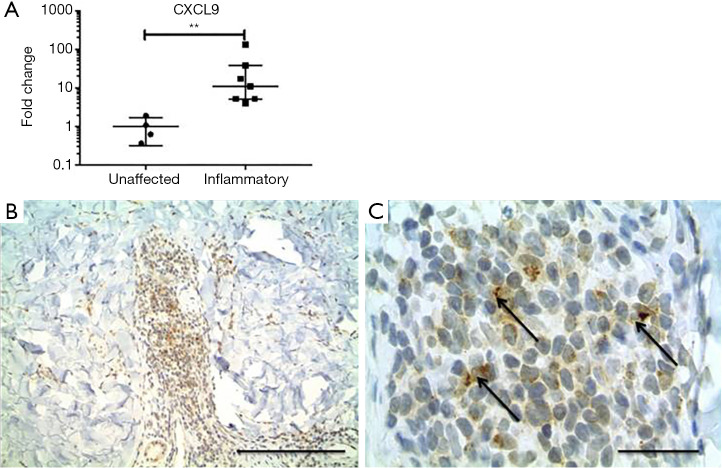
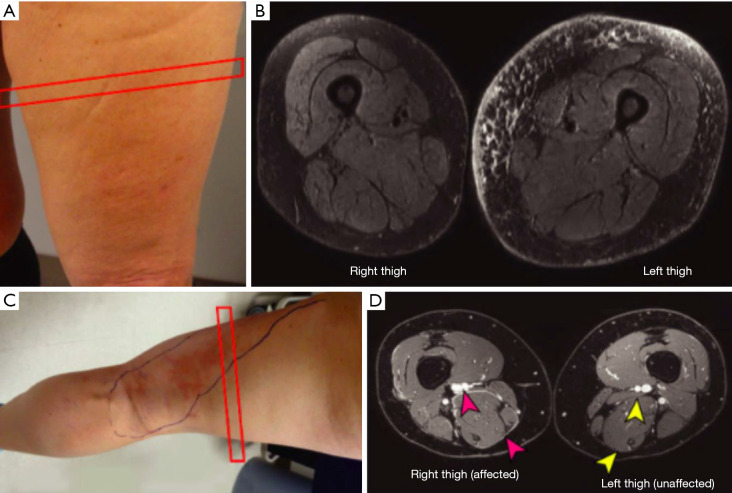
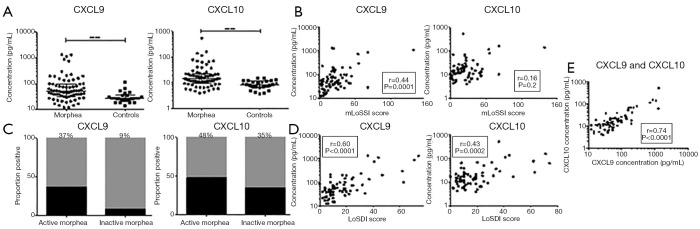
Morphea is a rare autoimmune condition causing inflammation and sclerosis of the skin and underlying soft tissue. It is characterized by periods of activity (inflammation admixed with fibrosis), ultimately resulting in permanent damage (pigment change and tissue loss). Damage resulting from unchecked activity can lead to devastating, permanent cosmetic and functional sequelae including hair loss; cutaneous, soft tissue and bony atrophy; joint contractures; and growth restriction of the affected body site in children. This makes the early identification of activity and initiation of appropriate treatment crucial to limiting damage in morphea. To this end, recent investigative work has focused on validation of clinical, biomarker, imaging, and histologic outcomes aimed at accurately quantifying activity and damage. Despite promising results, further work is needed to better validate these measures before they can be used in the clinic and research settings. Although there has been recent approval of less toxic, targeted therapies for many inflammatory skin conditions, none have been systematically investigated in morphea. The mainstays of treatment for active morphea are corticosteroids and methotrexate. These are often limited by substantial toxicity. The paucity of new treatments for morphea is the result of a lack of studies examining its pathogenesis, with many reviews extrapolating from research in systemic sclerosis. Recent studies have demonstrated the role of dysregulated immune and fibrotic pathways in the pathogenesis of morphea, particularly interferon (IFN) gamma related pathways. Active morphea lesions have been found to display an inflammatory morphea signature with CXCR3 receptor ligands, as well as a distinct fibrotic signature reflecting fibroblast activation and collagen production. CXCL9 and 10 have been associated with increased measures of disease activity. While immune dysfunction is thought to play the primary role in morphea pathogenesis, there are other factors that may also contribute, including genetic predisposition, environmental factors, and vascular dysregulation. There remains an essential need for further research to elucidate the pathogenesis of morphea and the mode of action of dysregulated upstream and downstream immune and fibrotic pathways. These studies will allow for the discovery of novel biomarkers and targets for therapeutic development.
Keywords: Localized scleroderma; evaluation; morphea; pathogenesis; treatment.
2021 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/atm-20-6222). The series “Rheumatologic Skin Disease” was commissioned by the editorial office without any funding or sponsorship. The authors have no other conflicts of interest to declare.
Figures
References
-
- Peterson LS, Nelson AM, Su WP, et al. The epidemiology of morphea (localized scleroderma) in Olmsted County 1960-1993. J Rheumatol 1997;24:73-80. - PubMed
-
- Knobler R, Moinzadeh P, Hunzelmann N, et al. European Dermatology Forum S1-guideline on the diagnosis and treatment of sclerosing diseases of the skin, Part 1: localized scleroderma, systemic sclerosis and overlap syndromes. J Eur Acad Dermatol Venereol 2017;31:1401-24. 10.1111/jdv.14458 - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials