

Measuring Cognitive Health in Ethnically Diverse Older Adults
- PMID: 33842969
- PMCID: PMC8824686
- DOI: 10.1093/geronb/gbab062
Measuring Cognitive Health in Ethnically Diverse Older Adults
Abstract
Objectives: Understanding racial/ethnic disparities in late-life cognitive health is a public health imperative. We used baseline data from the Kaiser Healthy Aging and Diverse Life Experiences (KHANDLE) study to examine how age, education, gender, and clinical diagnosis, a proxy for brain health, are associated with cross-sectional measures of cognition in diverse racial/ethnic groups.
Methods: Comprehensive measures of cognition were obtained using the Spanish and English Neuropsychological Assessment Scales and the National Institutes of Health Toolbox Cognitive Health Battery in a sample of 1,695 KHANDLE participants (Asians 24%, Blacks 26%, Latinos 20%, Whites 29%). A 25% random subsample was clinically evaluated and diagnosed with normal cognition, mild cognitive impairment (MCI), or dementia. Cognitive test scores were regressed on core demographic variables and diagnosis in the combined sample and in multiple group analyses stratified by racial/ethnic group.
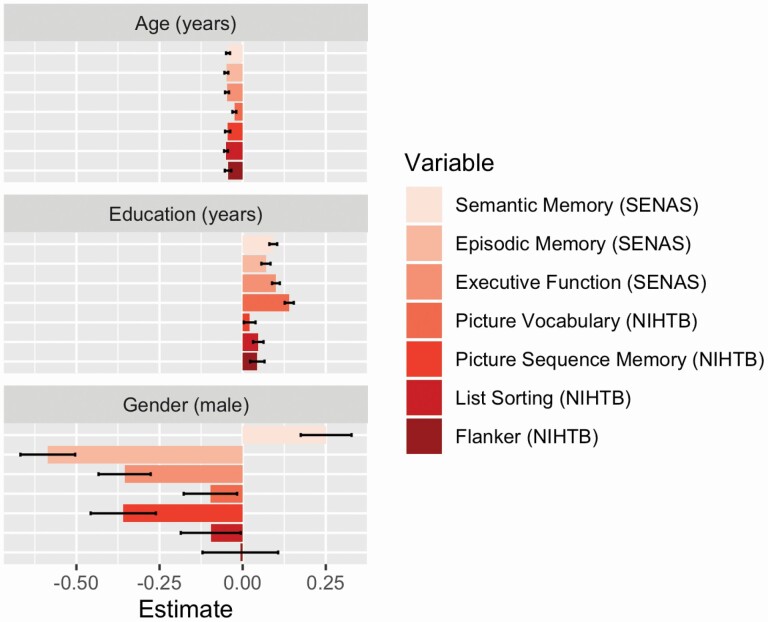
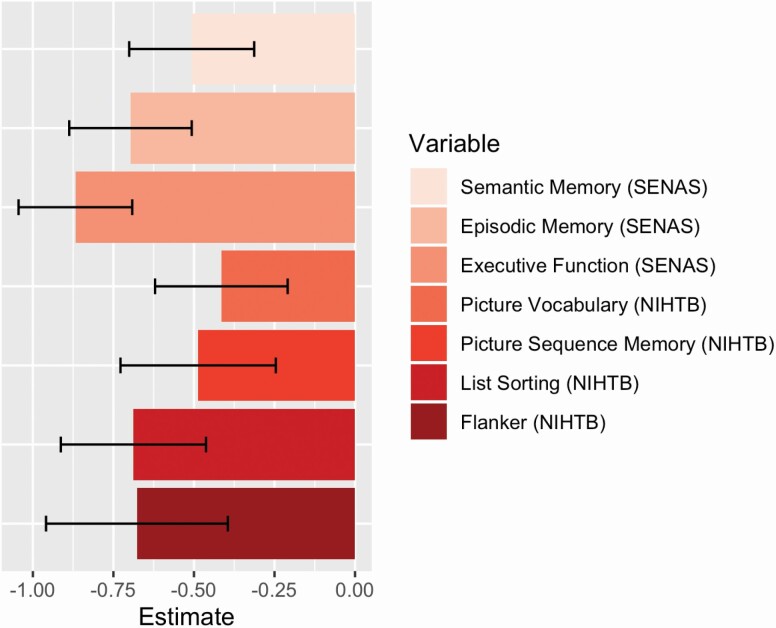
Results: Race/ethnicity and education were variably associated with test scores with strongest associations with tests of vocabulary and semantic memory. Older age was associated with poorer performance on all measures, and gender differences varied across cognitive tests. Clinical diagnosis of MCI or dementia was associated with average decrements in test scores that ranged from -0.41 to -0.84 SD, with largest differences on tests of executive function and episodic memory. With few exceptions, associations of demographic variables and clinical diagnosis did not differ across racial/ethnic groups.
Discussion: The robust associations of cognitive test results with clinical diagnosis independent of core demographic variables and race/ethnicity support the validity of cognitive tests as indicators for brain health in diverse older adults.
Keywords: Cognition; Cross-cultural differences; Epidemiology; Neuropsychology.
© The Author(s) 2021. Published by Oxford University Press on behalf of The Gerontological Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Besser, L., Kukull, W., Knopman, D. S., Chui, H., Galasko, D., Weintraub, S., Jicha, G., Carlsson, C., Burns, J., Quinn, J., Sweet, R. A., Rascovsky, K., Teylan, M., Beekly, D., Thomas, G., Bollenbeck, M., Monsell, S., Mock, C., Zhou, X. H., . . . Clinical Core leaders of the National Institute on Aging. (2018). Version 3 of the National Alzheimer’s Coordinating Center’s Uniform Data Set. Alzheimer Disease and Associated Disorders, 32(4), 351–358. doi: 10.1097/WAD.0000000000000279 - DOI - PMC - PubMed
-
- Blom, G. 1958. Statistical estimates and transformed beta-variables. Wiley.
-
- Brewster, P. W., Melrose, R. J., Marquine, M. J., Johnson, J. K., Napoles, A., MacKay-Brandt, A., Farias, S., Reed, B., & Mungas, D. (2014). Life experience and demographic influences on cognitive function in older adults. Neuropsychology, 28(6), 846–858. doi: 10.1037/neu0000098 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
