

Screening of postpartum diabetes in women with gestational diabetes: high-risk subgroups and areas for improvements-the STRONG observational study
- PMID: 33842997
- PMCID: PMC8316164
- DOI: 10.1007/s00592-021-01707-9
Screening of postpartum diabetes in women with gestational diabetes: high-risk subgroups and areas for improvements-the STRONG observational study
Erratum in
-
Correction to: Screening of postpartum diabetes in women with gestational diabetes: high‑risk subgroups and areas for improvements-the STRONG observational study.Acta Diabetol. 2021 Sep;58(9):1199. doi: 10.1007/s00592-021-01730-w. Acta Diabetol. 2021. PMID: 34117525 Free PMC article. No abstract available.
Abstract
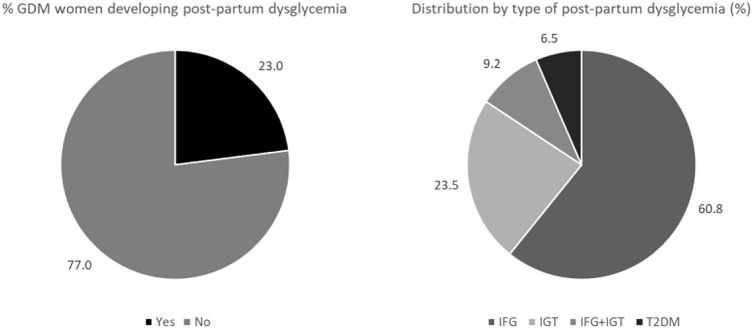
Aims: To assess the proportion of women with gestational diabetes (GDM) by performing postpartum Oral Glucose Tolerance Test (OGTT) and to identify GDM phenotypes at high-risk of postpartum dysglycemia (PPD).
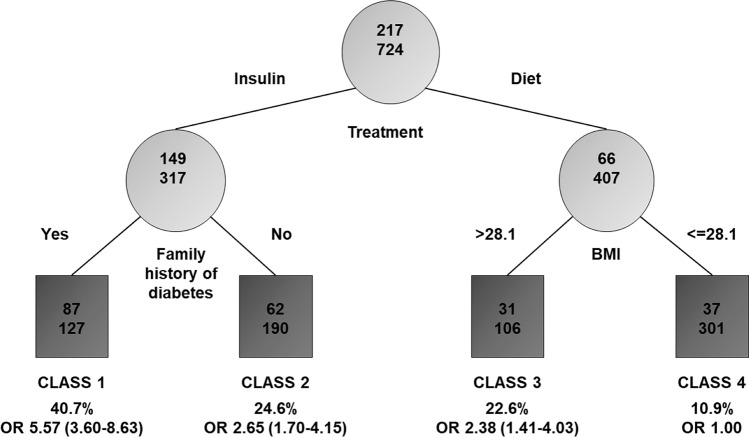
Methods: Observational, retrospective, multicenter study involving consecutive GDM women. Recursive partitioning (RECPAM) analysis was used to identify distinct and homogeneous subgroups of women at different PPD risk.
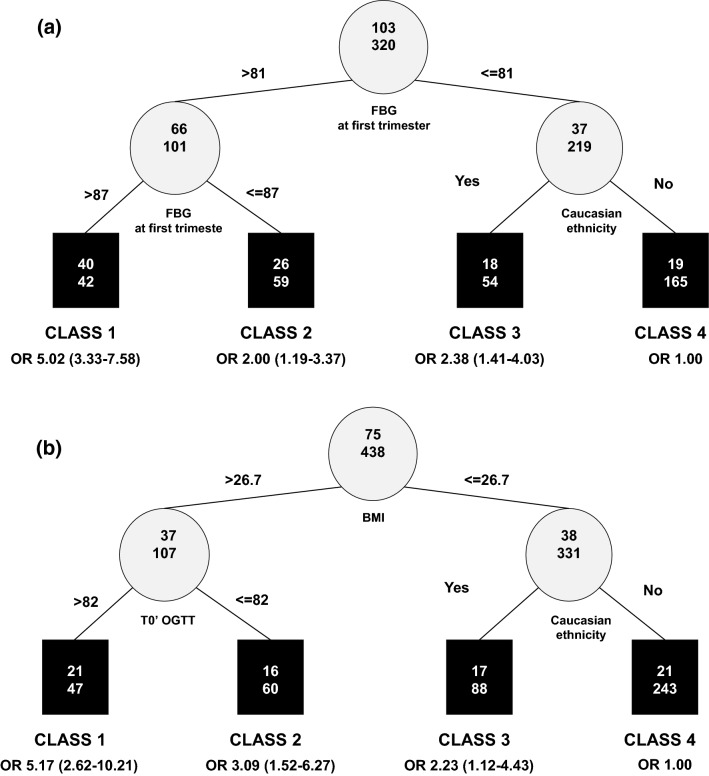
Results: From a sample of 2,736 women, OGTT was performed in 941 (34.4%) women, of whom 217 (23.0%) developed PPD. Insulin-treated women having family history of diabetes represented the subgroup with the highest PPD risk (OR 5.57, 95% CI 3.60-8.63) compared to the reference class (women on diet with pre-pregnancy BMI < = 28.1 kg/m2). Insulin-treated women without family diabetes history and women on diet with pre-pregnancy BMI > 28.1 kg/m2 showed a two-fold PPD risk. Previous GDM and socioeconomic status represent additional predictors. Fasting more than post-prandial glycemia plays a predictive role, with values of 81-87 mg/dl (4.5-4.8 mmol/l) (lower than the current diagnostic GDM threshold) being associated with PPD risk.
Conclusions: Increasing compliance to postpartum OGTT to prevent/delay PPD is a priority. Easily available characteristics identify subgroups of women more likely to benefit from preventive strategies. Fasting BG values during pregnancy lower than those usually considered deserve attention.
Keywords: Gestational diabetes; Obesity; Postpartum dysglycemia; Risk factors; Type 2 diabetes.
© 2021. The Author(s).
Conflict of interest statement
None.
Figures
References
-
- Lapolla A, Dalfra MG, Lencioni C, Di Cianni G. Epidemiology of diabetes in pregnancy: a review of Italian data. Diabetes Nutr Metab. 2004;17:358–367. - PubMed
-
- O’Sullivan EP, Avalos G, O’Reilly M, Dennedy MC, Gaffney G, Dunne F. Atlantic DIP Collaborators. Atlantic Diabetes in pregnancy (DIP): the prevalence and outcomes of gestational diabetes mellitus using new diagnostic criteria. Diabetologia. 2011;54:1670–1675. doi: 10.1007/s00125-011-2150-4. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
