

Comparative effectiveness of guselkumab in psoriatic arthritis: results from systematic literature review and network meta-analysis
- PMID: 33844022
- PMCID: PMC8121447
- DOI: 10.1093/rheumatology/keab119
Comparative effectiveness of guselkumab in psoriatic arthritis: results from systematic literature review and network meta-analysis
Abstract
Objective: The efficacy of the novel interleukin (IL)-23p19 inhibitor guselkumab for psoriatic arthritis (PsA) has recently been demonstrated in two phase 3 trials (DISCOVER-1 & -2) but has not been evaluated vs other targeted therapies for PsA. The objective was to compare guselkumab to targeted therapies for PsA for safety and joint and skin efficacy through network meta-analysis (NMA).
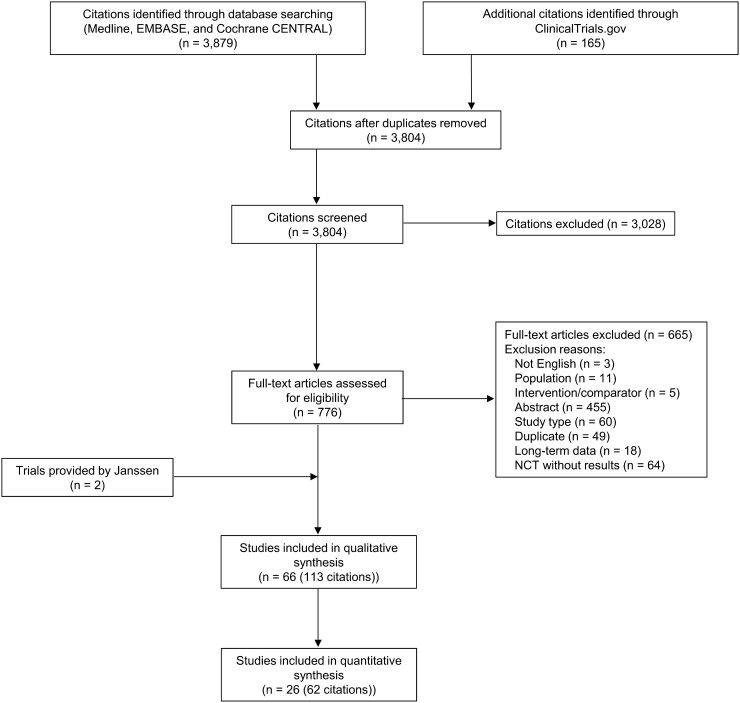
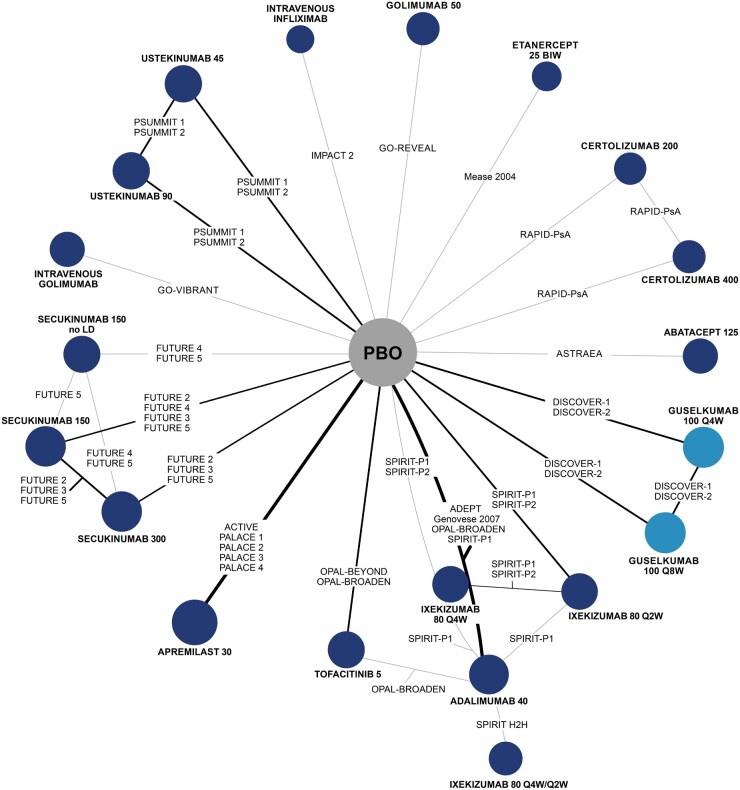
Methods: A systematic literature review was conducted in January 2020 to identify randomized controlled trials. Bayesian NMAs were performed to compare treatments on American College of Rheumatology (ACR) 20/50/70 response, mean change from baseline in van der Heijde-Sharp (vdH-S) score, Psoriasis Area Severity Index (PASI) 75/90/100 response, adverse events (AEs) and serious adverse events (SAEs).
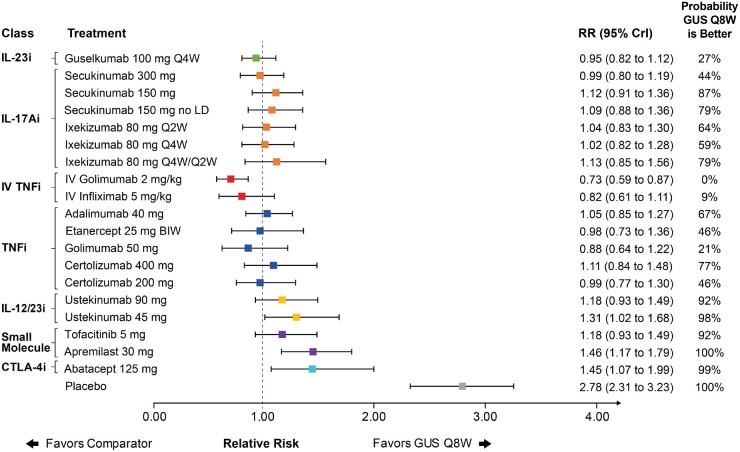
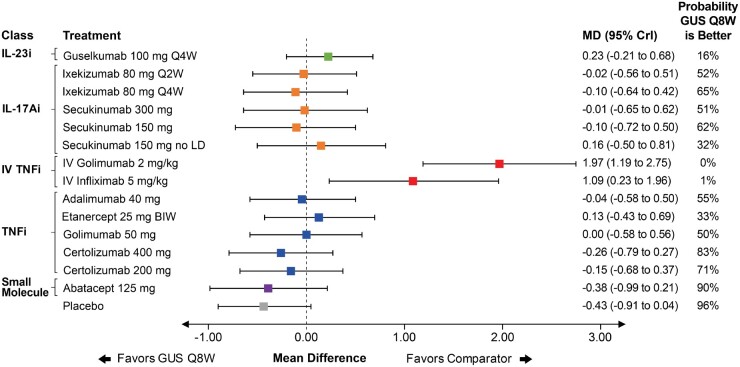
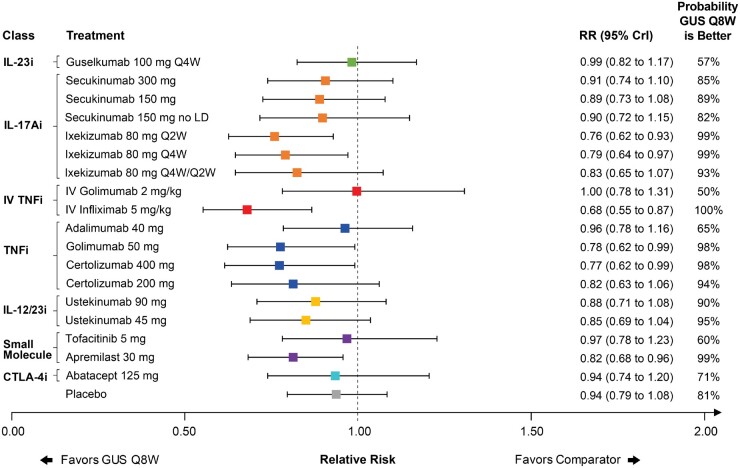
Results: Twenty-six phase 3 studies evaluating 13 targeted therapies for PsA were included. For ACR 20 response, guselkumab 100 mg every 8 weeks (Q8W) was comparable to IL-17A inhibitors and subcutaneous tumor necrosis factor (TNF) inhibitors. Similar findings were observed for ACR 50 and 70. For vdH-S score, guselkumab Q8W was comparable to other agents except intravenous TNF therapies. Results for PASI 75 and PASI 90 response suggested guselkumab Q8W was better than most other agents. For PASI 100, guselkumab Q8W was comparable to other active agents. For AEs and SAEs, guselkumab Q8W ranked highly but comparative conclusions were uncertain. Similar results were observed for all outcomes for guselkumab 100 mg every four weeks.
Conclusions: In this NMA, guselkumab demonstrated favorable arthritis efficacy comparable to IL-17A and subcutaneous TNF inhibitors while offering better PASI response relative to many other treatments.
Keywords: ACR; NMA; PASI; SLR; TNF; biologics; guselkumab; interleukin; psoriatic arthritis.
© The Author(s) 2021. Published by Oxford University Press on behalf of the British Society for Rheumatology.
Figures

Comment in
-
'Too much of a good thing': can network meta-analysis guide treatment decision-making in psoriatic arthritis?Rheumatology (Oxford). 2021 Jul 1;60(7):3042-3044. doi: 10.1093/rheumatology/keab329. Rheumatology (Oxford). 2021. PMID: 33792657 No abstract available.
References
-
- Gudu T, Gossec L.. Quality of life in psoriatic arthritis. Expert Rev Clin Immunol 2018;14:405–17. - PubMed
-
- McArdle A, Pennington S, FitzGerald O.. Clinical features of psoriatic arthritis: a comprehensive review of unmet clinical needs. Clin Rev Allergy Immunol 2018;55:271–94. - PubMed
-
- Ritchlin CT, Colbert RA, Gladman DD.. Psoriatic arthritis. N Engl J Med 2017;376:957–70. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
