

Longitudinal assessment of IFN-I activity and immune profile in critically ill COVID-19 patients with acute respiratory distress syndrome
- PMID: 33845874
- PMCID: PMC8040759
- DOI: 10.1186/s13054-021-03558-w
Longitudinal assessment of IFN-I activity and immune profile in critically ill COVID-19 patients with acute respiratory distress syndrome
Abstract
Background: Since the onset of the pandemic, only few studies focused on longitudinal immune monitoring in critically ill COVID-19 patients with acute respiratory distress syndrome (ARDS) whereas their hospital stay may last for several weeks. Consequently, the question of whether immune parameters may drive or associate with delayed unfavorable outcome in these critically ill patients remains unsolved.
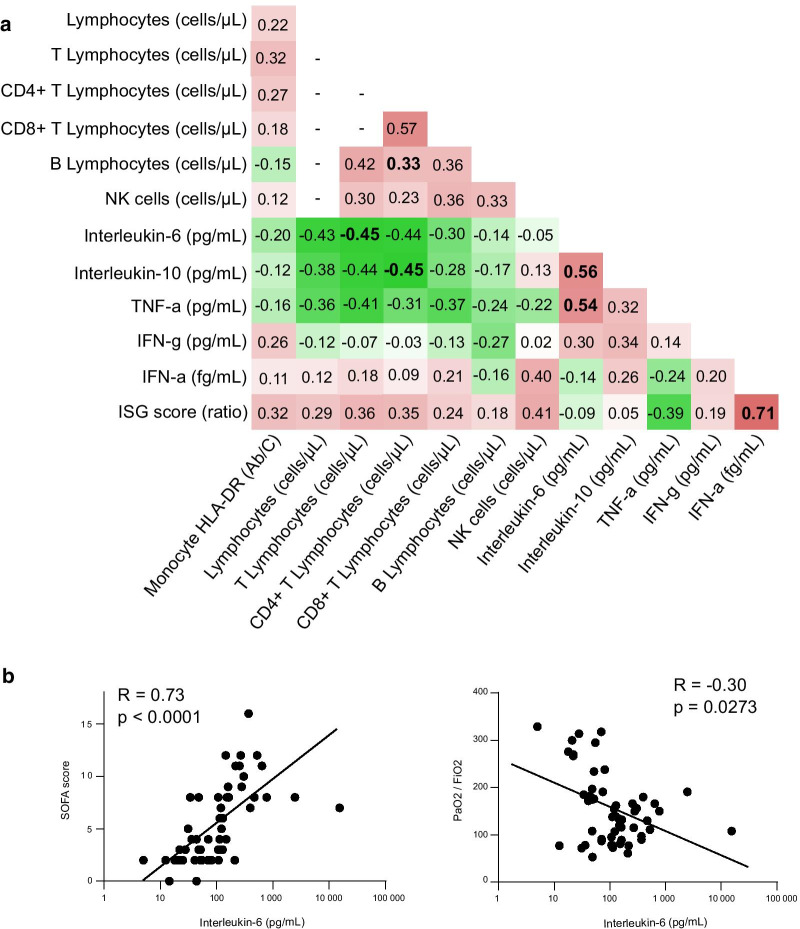
Methods: We present a dynamic description of immuno-inflammatory derangements in 64 critically ill COVID-19 patients including plasma IFNα2 levels and IFN-stimulated genes (ISG) score measurements.
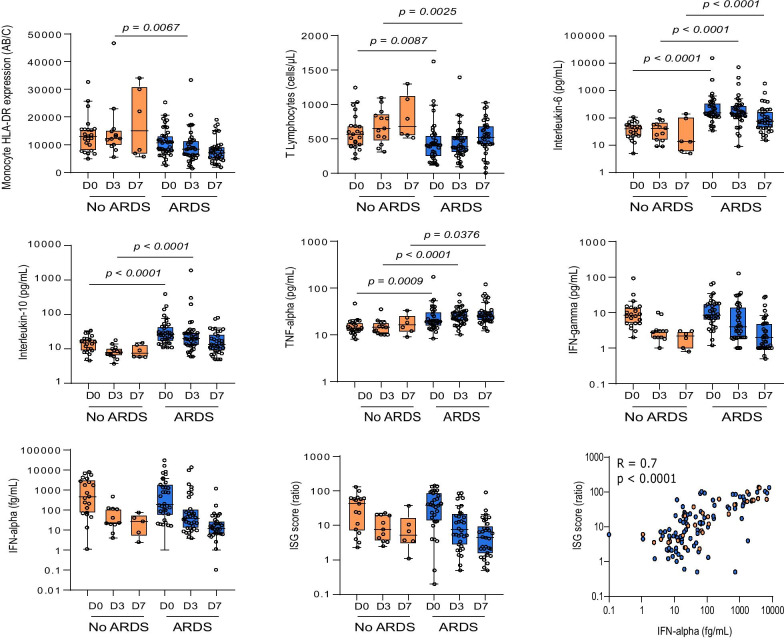
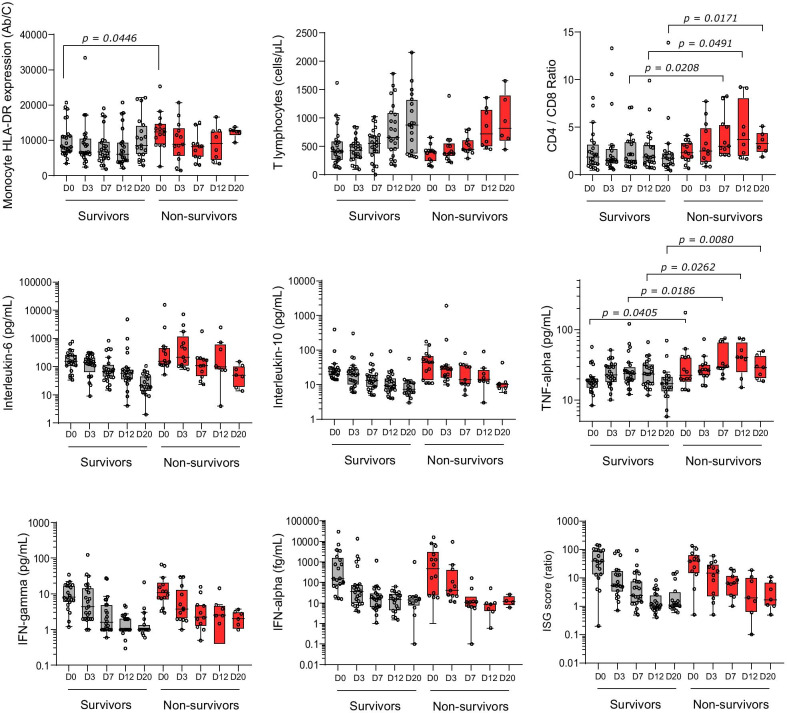
Results: ARDS patients presented with persistently decreased lymphocyte count and mHLA-DR expression and increased cytokine levels. Type-I IFN response was initially induced with elevation of IFNα2 levels and ISG score followed by a rapid decrease over time. Survivors and non-survivors presented with apparent common immune responses over the first 3 weeks after ICU admission mixing gradual return to normal values of cellular markers and progressive decrease of cytokines levels including IFNα2. Only plasma TNF-α presented with a slow increase over time and higher values in non-survivors compared with survivors. This paralleled with an extremely high occurrence of secondary infections in COVID-19 patients with ARDS.
Conclusions: Occurrence of ARDS in response to SARS-CoV2 infection appears to be strongly associated with the intensity of immune alterations upon ICU admission of COVID-19 patients. In these critically ill patients, immune profile presents with similarities with the delayed step of immunosuppression described in bacterial sepsis.
Keywords: ARDS; COVID-19; Immune profile; Immunosuppression; Type-I IFN.
Conflict of interest statement
The authors declare no competing financial interests in relation to the work.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
