

Distinct cellular immune profiles in the airways and blood of critically ill patients with COVID-19
- PMID: 33846275
- PMCID: PMC8050882
- DOI: 10.1136/thoraxjnl-2020-216256
Distinct cellular immune profiles in the airways and blood of critically ill patients with COVID-19
Abstract
Background: Knowledge of the pathophysiology of COVID-19 is almost exclusively derived from studies that examined the immune response in blood. We here aimed to analyse the pulmonary immune response during severe COVID-19 and to compare this with blood responses.
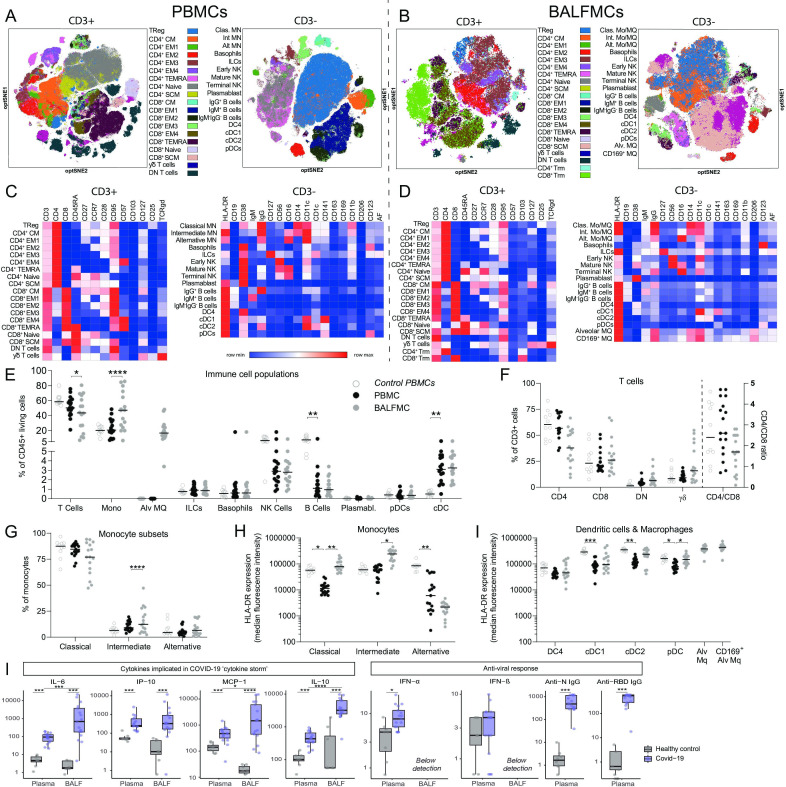
Methods: This was an observational study in patients with COVID-19 admitted to the intensive care unit (ICU). Mononuclear cells were purified from bronchoalveolar lavage fluid (BALF) and blood, and analysed by spectral flow cytometry; inflammatory mediators were measured in BALF and plasma.
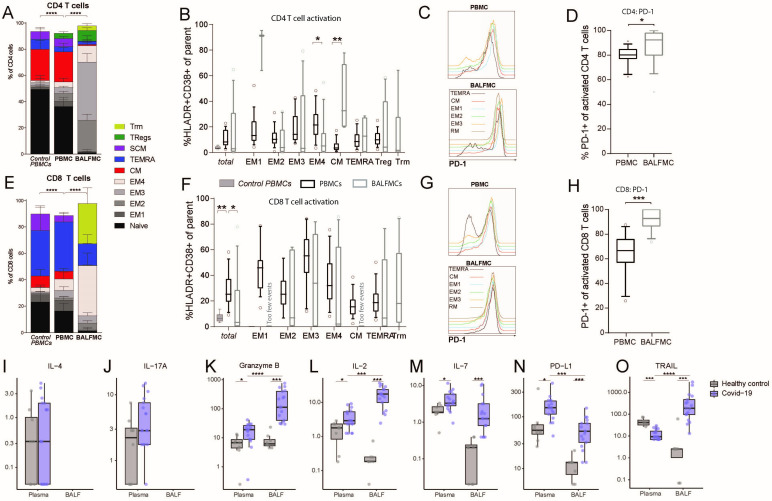
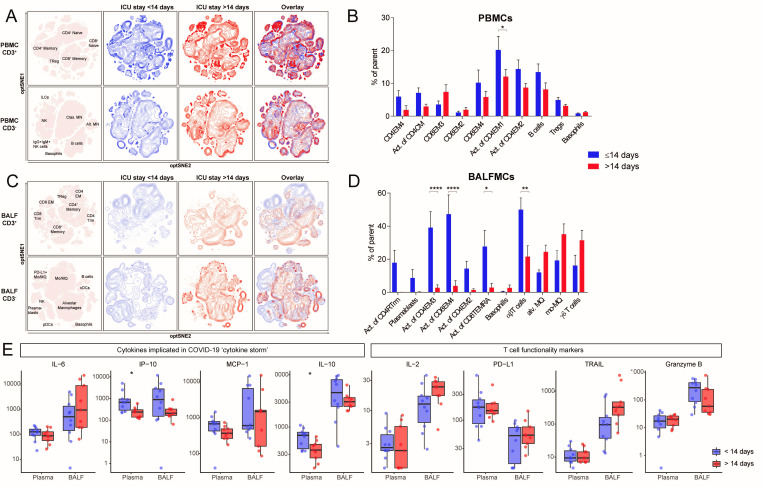
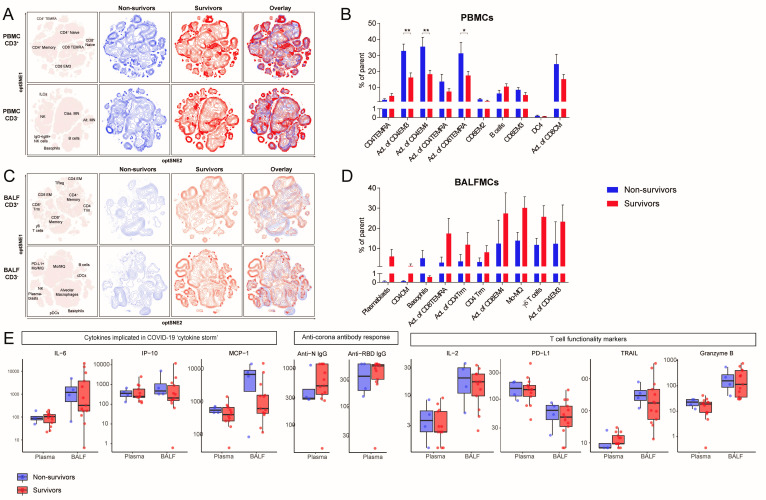
Findings: Paired blood and BALF samples were obtained from 17 patients, four of whom died in the ICU. Macrophages and T cells were the most abundant cells in BALF, with a high percentage of T cells expressing the ƴδ T cell receptor. In the lungs, both CD4 and CD8 T cells were predominantly effector memory cells (87·3% and 83·8%, respectively), and these cells expressed higher levels of the exhaustion marker programmad death-1 than in peripheral blood. Prolonged ICU stay (>14 days) was associated with a reduced proportion of activated T cells in peripheral blood and even more so in BALF. T cell activation in blood, but not in BALF, was higher in fatal COVID-19 cases. Increased levels of inflammatory mediators were more pronounced in BALF than in plasma.
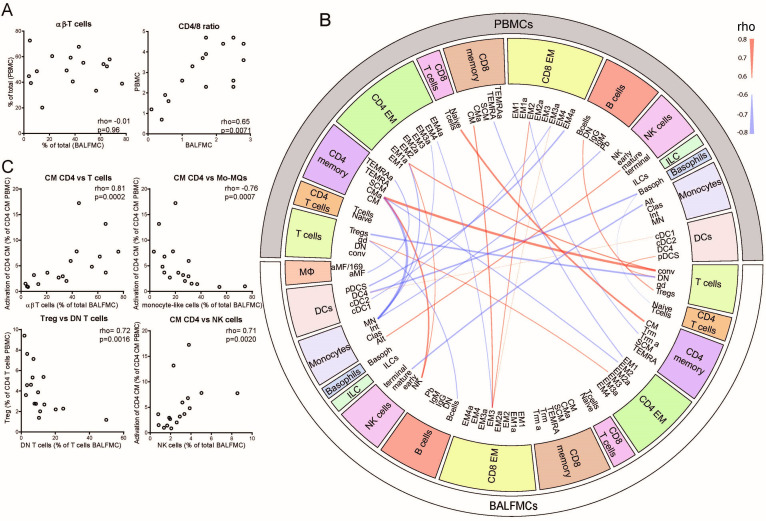
Interpretation: The bronchoalveolar immune response in COVID-19 has a unique local profile that strongly differs from the immune profile in peripheral blood. Fully elucidating COVID-19 pathophysiology will require investigation of the pulmonary immune response.
Keywords: COVID-19; pneumonia; respiratory infection; viral infection.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Immune responses to SARS-CoV-2 in the lung.Thorax. 2021 Oct;76(10):961. doi: 10.1136/thoraxjnl-2021-217231. Epub 2021 Jun 4. Thorax. 2021. PMID: 34088785 No abstract available.
References
-
- WHO - Coronavirus disease (COVID-19) pandemic. Available: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 [Accessed 18 Jan 2021].
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials