Octogenarian newly diagnosed multiple myeloma patients without geriatric impairments: the role of age >80 in the IMWG frailty score
- PMID: 33846296
- PMCID: PMC8041817
- DOI: 10.1038/s41408-021-00464-w
Octogenarian newly diagnosed multiple myeloma patients without geriatric impairments: the role of age >80 in the IMWG frailty score
Conflict of interest statement
M.D. has received honoraria for lectures from Sanofi and GSK; has served on the advisory boards for GSK. A.L. has received honoraria from Amgen, Bristol-Myers Squibb, Celgene, Janssen, and GSK; has served on the advisory boards for Bristol-Myers Squibb, Celgene, Janssen, and Takeda. M.O. has received honoraria from Amgen, Bristol-Myers Squibb, Celgene, Janssen, GSK, Sanofi, and Takeda; has served on the advisory boards for Amgen, Bristol-Myers Squibb, Celgene, Janssen, GSK, Sanofi, and Takeda. A.M.L. has received personal fees from Incyte; has received research funding from Novartis, Janssen, AbbVie, Roche, Celgene, Amgen, Bristol-Myers Squibb, Takeda, Incyte, Pfizer, Beigene, Oncopeptides, Verastem, Karyopharm, Archigen, Biopharma, Debiopharm, Morphosys, Fibrogen, and Onconova. G.G. has served on the advisory boards for Janssen, AbbVie, and AstraZeneca; has served on the speaker’s bureaus for Janssen and AbbVie. M.T.P. has received honoraria from and served on the advisory boards for Celgene, Janssen-Cilag, Amgen, Bristol-Myers Squibb, Takeda, Sanofi, and GSK. R.Z. has served on the advisory boards for Janssen and Celgene. F.P. has served on the advisory boards for Celgene and Janssen. G.B. has received honoraria from Novartis, Celgene Amgen, and Takeda. N.G. has received research grants from Celgene and Janssen Pharmaceutica; has received sponsorship for clinical studies from Janssen Pharmaceutica, Millennium Pharmaceuticals, and GSK; has served on the advisory boards for Celgene, Takeda, and Janssen Pharmaceutica; has received support for participating in meetings from Janssen Pharmaceutica, Celgene, and Bristol-Myers Squibb. F.D.R. has received honoraria from Celgene, Janssen, Amgen, and Takeda. P.C. has participated as a lecturer and/or has served on the advisory boards for AbbVie, ADC Therapeutics, Amgen, Celgene, Daiichi Sankyo, Gilead, Incyte, Janssen, Jazz Pharmaceuticals, Kite, Kyowa Kirin, Novartis, Roche, Sanofi, Servier, and Takeda. P.M. has received honoraria and/or served on the scientific advisory boards for Celgene, Janssen, Takeda, Bristol-Myers Squibb, Amgen, Novartis, Gilead, Jazz, Sanofi, AbbVie, and Glaxo-Smith-Kline. R.H. has had a consultant or advisory relationship with Janssen, Amgen, Celgene, AbbVie, BMS, Novartis, PharmaMar, and Takeda; has received honoraria from Janssen, Amgen, Celgene, BMS, PharmaMar, and Takeda; has received research funding from Janssen, Amgen, Celgene, BMS, Novartis, and Takeda. P.S. has served on the advisory boards for Amgen, Celgene, Genenta, Janssen, Seattle Genetics, Takeda, and Karyopharm. M.B. has received honoraria from Sanofi, Celgene, Amgen, Janssen, Novartis, Bristol-Myers Squibb, and AbbVie; has served on the advisory boards for Janssen and GSK; has received research funding from Sanofi, Celgene, Amgen, Janssen, Novartis, Bristol-Myers Squibb, and Mundipharma. S.B. has received honoraria from Celgene, Amgen, Janssen, and Bristol-Myers Squibb; has served on the advisory boards for Celgene, Amgen, Janssen, and Karyopharm; has received consultancy fees from Janssen and Takeda. The remaining authors declare no competing interests.
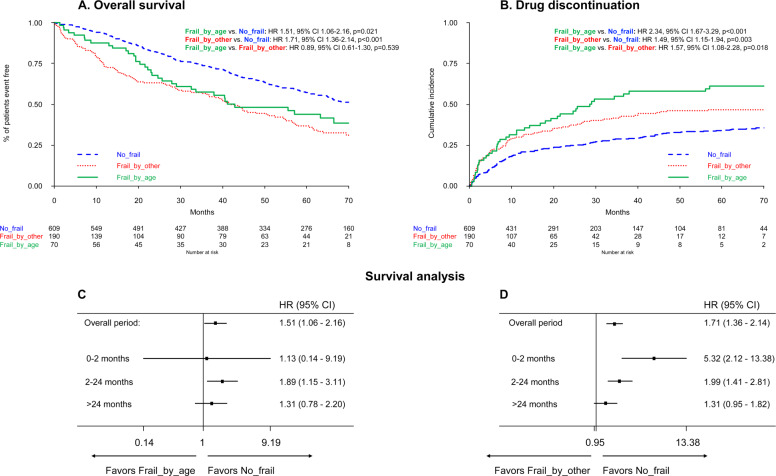
Figures