

Abnormal myocardial work in children with Kawasaki disease
- PMID: 33846402
- PMCID: PMC8042008
- DOI: 10.1038/s41598-021-86933-5
Abnormal myocardial work in children with Kawasaki disease
Abstract
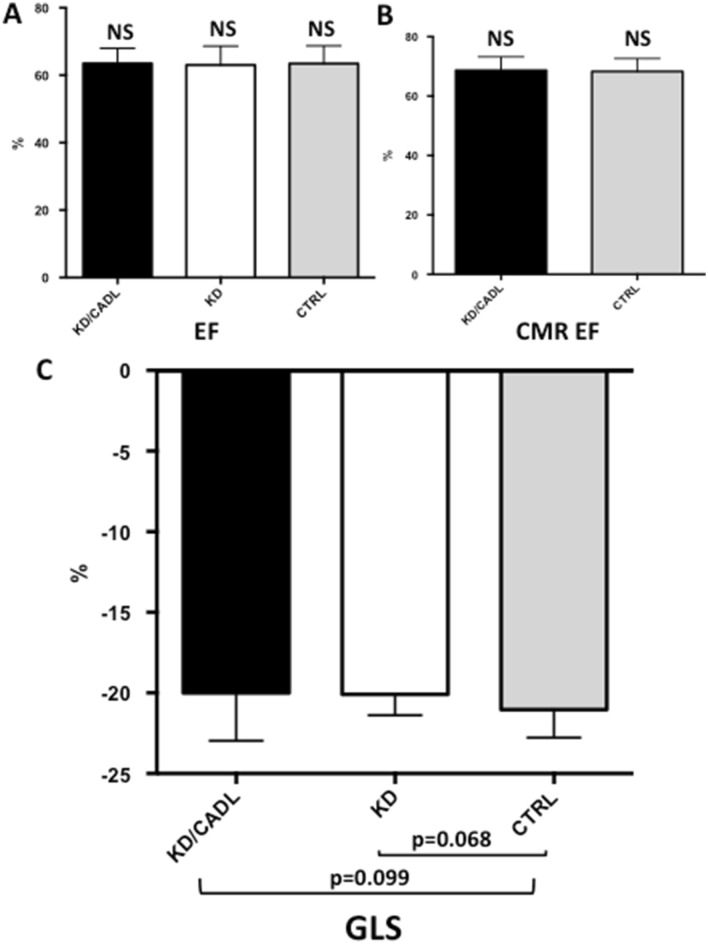
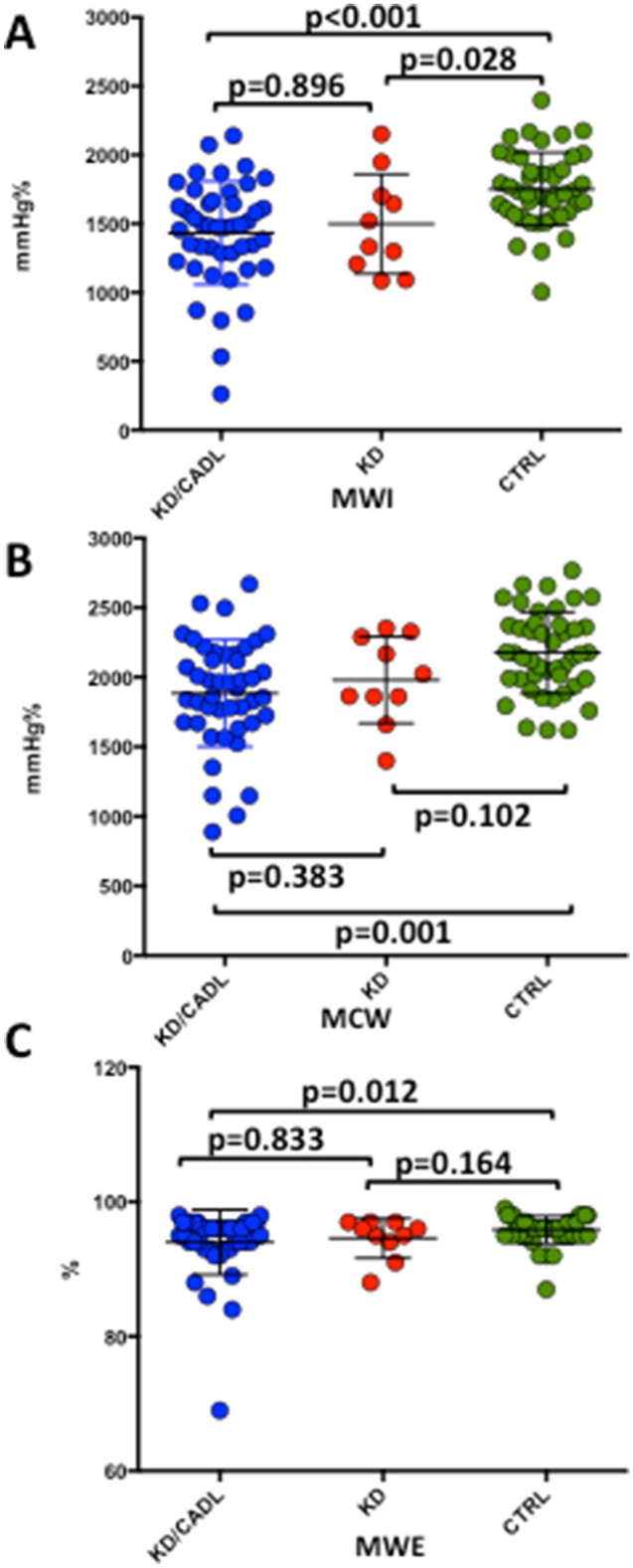
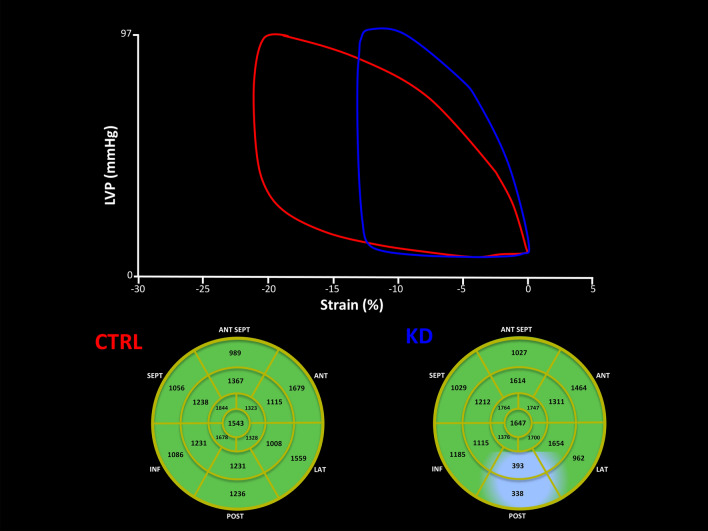
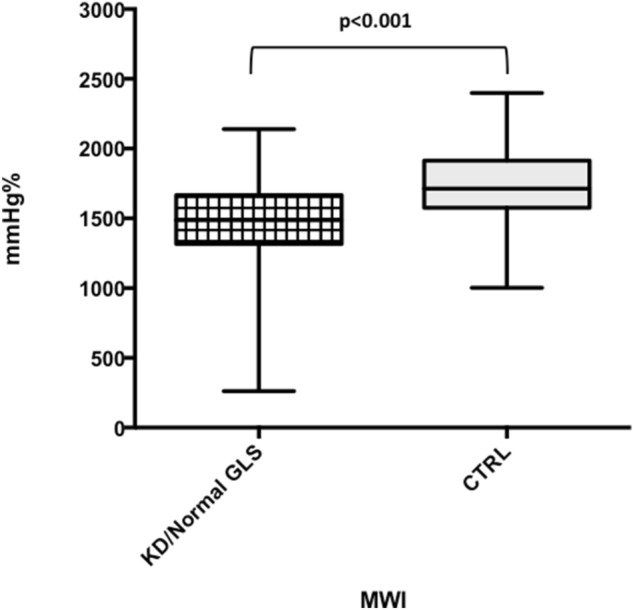
Kawasaki disease (KD) can be associated with high morbidity and mortality due to coronary artery aneurysms formation and myocardial dysfunction. Aim of this study was to evaluate the diagnostic performance of non-invasive myocardial work in predicting subtle myocardial abnormalities in Kawasaki disease (KD) children with coronary dilatation (CADL). A total of 100 patients (age 8.7 ± 5 years) were included: 45 children with KD and CADL (KD/CADL) (Z-score > 2.5), 45 age-matched controls (CTRL) and, finally, an additional group of 10 children with KD in absence of coronary dilatation (KD group). Left ventricular (LV) systolic function and global longitudinal strain (GLS) were assessed. Global myocardial work index (MWI) was calculated as the area of the LV pressure-strain loops. From MWI, global Constructive Work (MCW), Wasted Work (MWW) and Work Efficiency (MWE) were estimated. Despite normal LV systolic function by routine echocardiography, KD/CADL patients had lower MWI (1433.2 ± 375.8 mmHg% vs 1752.2 ± 265.7 mmHg%, p < 0.001), MCW (1885.5 ± 384.2 mmHg% vs 2175.9 ± 292.4 mmHg%, p = 0.001) and MWE (994.0 ± 4.8% vs 95.9 ± 2.0%, p = 0.030) compared to CTRL. Furthermore, MWI was significantly reduced in children belonging to the KD group in comparison with controls (KD: 1498.3 ± 361.7 mmHg%; KD vs CTRL p = 0.028) and was comparable between KD/CADL and KD groups (KD/CADL vs KD p = 0.896). Moreover, KD/CADL patients with normal GLS (n = 38) preserved significant differences in MWI and MCW in comparison with CTRL. MWI, MCW and MWE were significantly reduced in KD children despite normal LVEF and normal GLS. These abnormalities seems independent from CADL. Thus, in KD with normal LVEF and normal GLS, estimation of MWI may be a more sensitive indicator of myocardial dysfunction.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
