

Malaria Infection Is Common and Associated With Perinatal Mortality and Preterm Delivery Despite Widespread Use of Chemoprevention in Mali: An Observational Study 2010 to 2014
- PMID: 33846719
- PMCID: PMC8528392
- DOI: 10.1093/cid/ciab301
Malaria Infection Is Common and Associated With Perinatal Mortality and Preterm Delivery Despite Widespread Use of Chemoprevention in Mali: An Observational Study 2010 to 2014
Abstract
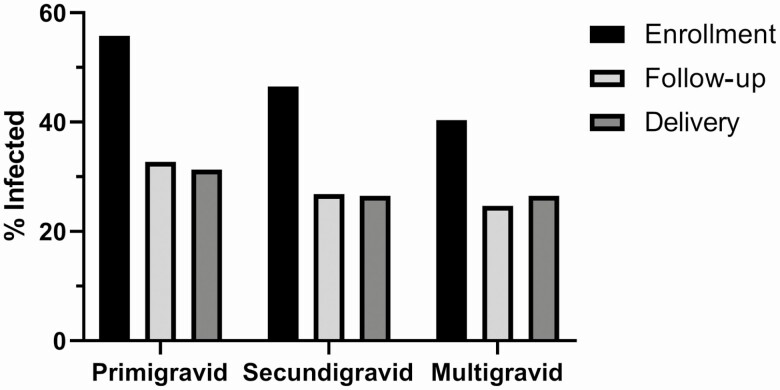
Background: In malaria-endemic areas, pregnant women and especially first-time mothers are more susceptible to Plasmodium falciparum. Malaria diagnosis is often missed during pregnancy, because many women with placental malaria remain asymptomatic or have submicroscopic parasitemia, masking the association between malaria and pregnancy outcomes. Severe maternal anemia and low birthweight deliveries are well-established sequelae, but few studies have confirmed the relationship between malaria infection and severe outcomes like perinatal mortality in high transmission zones.
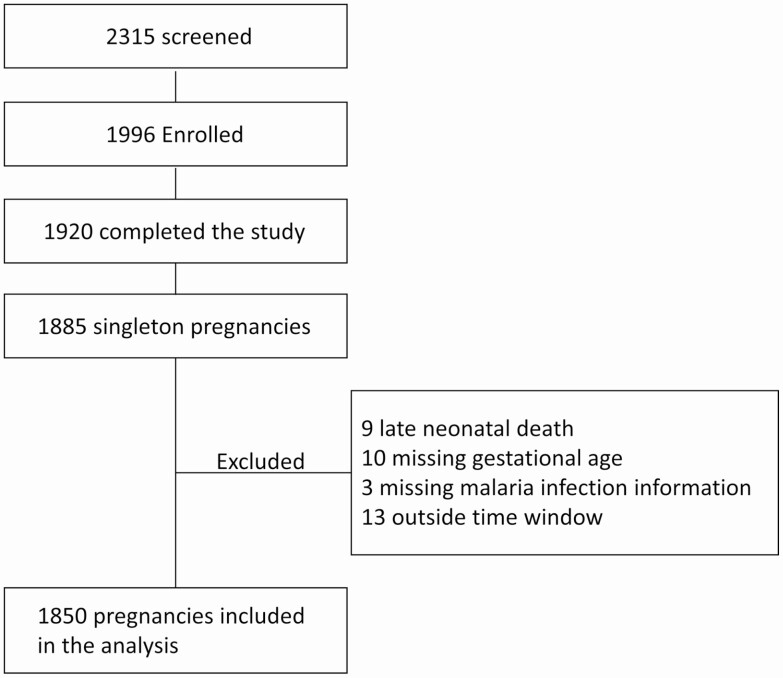
Methods: Pregnant women of any gestational age enrolled at antenatal clinic into a longitudinal cohort study in Ouelessebougou, Mali, an area of high seasonal malaria transmission. Follow-up visits included scheduled and unscheduled visits throughout pregnancy. Blood smear microscopy and polymerase chain reaction (PCR) analysis were employed to detect both microscopic and submicroscopic infections, respectively. Intermittent preventative treatment in pregnancy with sulfadoxine-pyrimethamine (IPTp-SP) was documented and prompt treatment regardless of symptoms given upon malaria diagnosis.
Results: Of the 1850 women followed through delivery, 72.6% of women received 2 or more IPTp-SP doses, 67.2% of women experienced at least 1 infection between enrollment up to and including delivery. Malaria infection increased the risks of stillbirth (adjusted hazard ratio [aHR] 3.87, 95% confidence interval [CI]: 1.18-12.71) and preterm delivery (aHR 2.41, 95% CI: 1.35-4.29) in primigravidae, and early neonatal death (death within 7 days) in secundigravidae and multigravidae (aHR 6.30, 95% CI: 1.41-28.15).
Conclusions: Malaria treatment after diagnosis, alongside IPTp-SP, is insufficient to prevent malaria-related stillbirth, early neonatal death and preterm delivery (PTD). Although IPTp-SP was beneficial in Mali during the study period, new tools are needed to improve pregnancy outcomes.
Clinical trials registration: NCT01168271.
Keywords: early neonatal death; intermittent preventative treatment in pregnancy; pregnancy malaria; preterm delivery; stillbirth.
Published by Oxford University Press for the Infectious Diseases Society of America 2021.
Figures
References
-
- Desai M, ter Kuile FO, Nosten F, et al. . Epidemiology and burden of malaria in pregnancy. Lancet Infect Dis 2007; 7:93–104. - PubMed
-
- Fried M, Nosten F, Brockman A, Brabin BJ, Duffy PE. Maternal antibodies block malaria. Nature 1998; 395:851–2. - PubMed
-
- WHO. World malaria report. Available at: https://www.who.int/publications-detail/world-malaria-report-2019. Accessed December 2020.
-
- Tako EA, Zhou A, Lohoue J, Leke R, Taylor DW, Leke RF. Risk factors for placental malaria and its effect on pregnancy outcome in Yaounde, Cameroon. Am J Trop Med Hyg 2005; 72:236–42. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
