

Predictive Role of Endoscopic Surveillance after Total Gastrectomy with R0 Resection for Gastric Cancer
- PMID: 33847079
- PMCID: PMC8042482
- DOI: 10.3346/jkms.2021.36.e88
Predictive Role of Endoscopic Surveillance after Total Gastrectomy with R0 Resection for Gastric Cancer
Abstract
Background: Endoscopic surveillance after total gastrectomy (TG) for gastric cancer is routinely performed to detect tumor recurrence and postoperative adverse events. However, the reports on the clinical benefits of endoscopic surveillance are ambiguous. We investigated the clinical benefit of endoscopic surveillance after TG for gastric cancer.
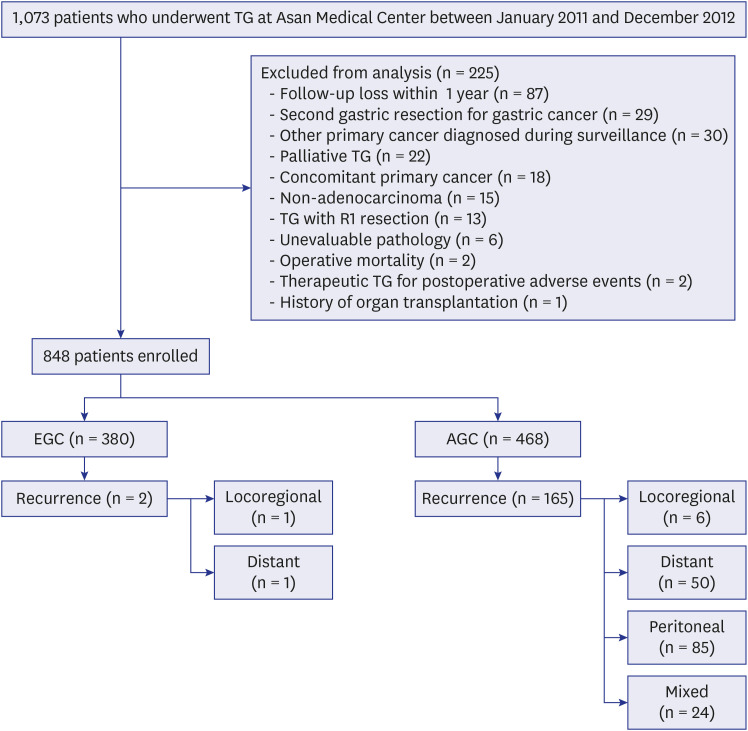
Methods: We analyzed 848 patients who underwent TG with R0 resection for gastric cancer between 2011 and 2012 (380 early gastric cancer and 468 advanced gastric cancer) and underwent regular postoperative surveillance with endoscopy and abdominopelvic computed tomography (CT) with contrast.
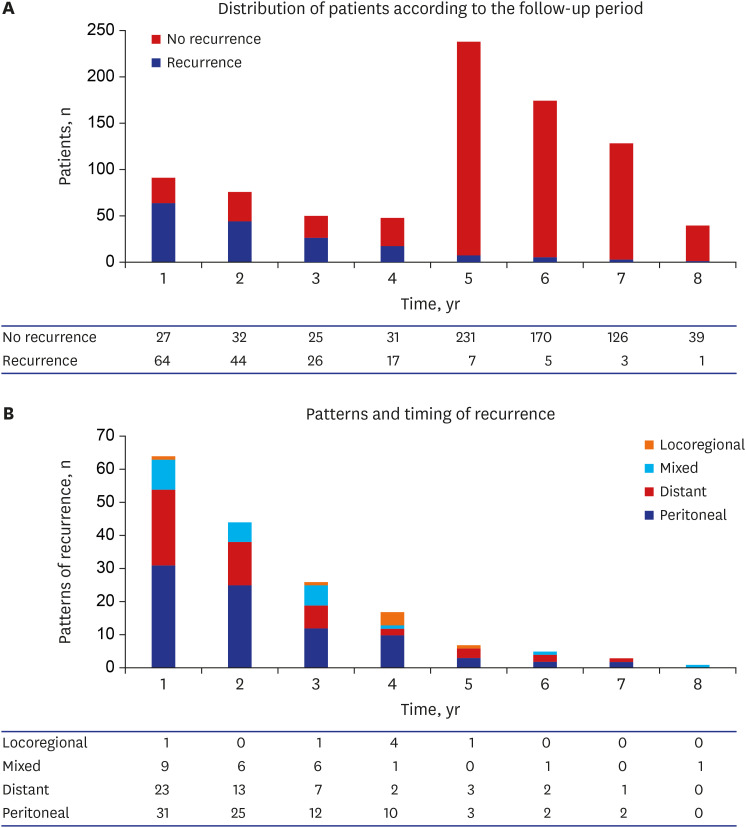
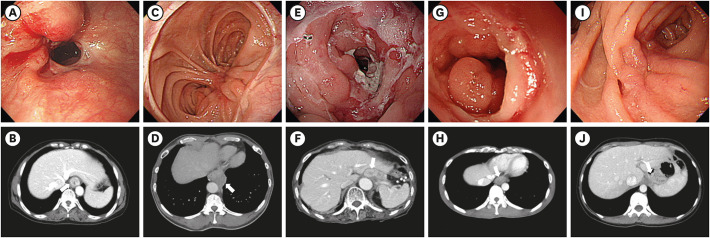
Results: Median follow-up periods were 58 months for both endoscopy (range, 3-96) and abdominopelvic CT (range, 1-96). Tumor recurrence occurred in 167 patients (19.7%), of whom seven (4.2%) were locoregional recurrences in the peri-anastomotic area (n = 5) or regional gastric lymph nodes (n = 2). Whereas the peri-anastomotic recurrences were detected by both endoscopy and abdominopelvic CT, regional lymph node recurrences were only detected by abdominopelvic CT. Out of the 23 events of postoperative adverse events, the majority (87%) were detected by radiologic examinations; three events of benign strictures in the anastomotic site were detected only by endoscopy.
Conclusion: Endoscopic surveillance did not have a significant role in detecting locoregional tumor recurrence and postoperative adverse events after TG with R0 resection for gastric cancer. Routine endoscopic surveillance after TG may be considered optional and performed according to the capacities of each clinical setting.
Keywords: Endoscopy; Gastric Cancer; Locoregional Recurrence; Postoperative Adverse Events; Surveillance; Total Gastrectomy.
© 2021 The Korean Academy of Medical Sciences.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. - PubMed
-
- Ferro A, Peleteiro B, Malvezzi M, Bosetti C, Bertuccio P, Levi F, et al. Worldwide trends in gastric cancer mortality (1980-2011), with predictions to 2015, and incidence by subtype. Eur J Cancer. 2014;50(7):1330–1344. - PubMed
-
- Wong BC, Lam SK, Wong WM, Chen JS, Zheng TT, Feng RE, et al. Helicobacter pylori eradication to prevent gastric cancer in a high-risk region of China: a randomized controlled trial. JAMA. 2004;291(2):187–194. - PubMed
-
- Park HA, Nam SY, Lee SK, Kim SG, Shim KN, Park SM, et al. The Korean guideline for gastric cancer screening. J Korean Med Assoc. 2015;58(5):373–384.
-
- Hamashima C, Shibuya D, Yamazaki H, Inoue K, Fukao A, Saito H, et al. The Japanese guidelines for gastric cancer screening. Jpn J Clin Oncol. 2008;38(4):259–267. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
