

Repeat stereotactic radiosurgery for progressive vestibular schwannomas after previous radiosurgery: a systematic review and meta-analysis
- PMID: 33847846
- PMCID: PMC8592961
- DOI: 10.1007/s10143-021-01528-y
Repeat stereotactic radiosurgery for progressive vestibular schwannomas after previous radiosurgery: a systematic review and meta-analysis
Abstract
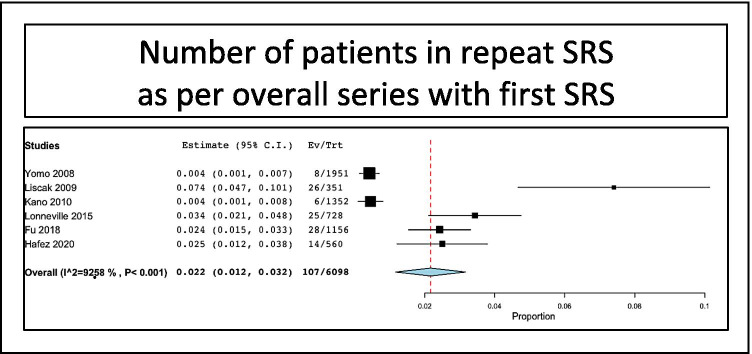
Vestibular schwannomas (VS) are slow-growing intracranial extraaxial benign tumors, developing from the vestibular part of the eight cranial nerves. Stereotactic radiosurgery (SRS) has now a long-term scientific track record as first intention treatment for small- to medium-sized VS. Though its success rate is very high, SRS for VS might fail to control tumor growth in some cases. However, the literature on repeat SRS after previously failed SRS remains scarce and reported in a low number of series with a limited number of cases. Here, we aimed at performing a systematic review and meta-analysis of the literature on repeat SRS for VS. Using PRISMA guidelines, we reviewed manuscripts published between January 1990 and October 2020 and referenced in PubMed. Tumor control and cranial nerve outcomes were evaluated with separate meta-analyses. Eight studies comprising 194 patients were included. The overall rate of patients treated in repeat SRS series as per overall series with first SRS was 2.2% (range 1.2-3.2%, p < 0.001). The mean time between first and second SRS was 50.7 months (median 51, range 44-64). The median marginal dose prescribed at first SRS was 12 Gy (range 8-24) and at second SRS was 12 Gy (range 9.8-19). After repeat SRS, tumor stability was reported in 61/194 patients, i.e., a rate of 29.6% (range 20.2-39%, I2 = 49.1%, p < 0.001). Tumor decrease was reported in 83/194 patients, i.e., a rate of 54.4% (range 33.7-75.1%, I2 = 89.1%, p < 0.001). Tumor progression was reported in 50/188 patients, i.e., a rate of 16.1% (range 2.5-29.7%, I2 = 87.1%, p = 0.02), rarely managed surgically. New trigeminal numbness was reported in 27/170 patients, i.e., a rate of 9.9% (range 1.4-18.3%, p < 0.02). New facial nerve palsy of worsened of previous was reported in 8/183 patients, i.e., a rate of 4.3% (range 1.4-7.2%, p = 0.004). Hearing loss was reported in 12/22 patients, i.e., a rate of 54.3% (range 24.8-83.8%, I2 = 70.7%, p < 0.001). Repeat SRS after previously failed SRS for VS is associated with high tumor control rates. Cranial nerve outcomes remain favorable, particularly for facial nerve. The rate of hearing loss appears similar to the one related to first SRS.
Keywords: Cochlear nerve; Facial nerve; Gamma Knife; Hearing; Stereotactic radiosurgery; Vestibular schwannoma.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Boari N, Bailo M, Gagliardi F, Franzin A, Gemma M, del Vecchio A, Bolognesi A, Picozzi P, Mortini P. Gamma Knife radiosurgery for vestibular schwannoma: clinical results at long-term follow-up in a series of 379 patients. J Neurosurg. 2014;121(Suppl):123–142. doi: 10.3171/2014.8.GKS141506. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
