

Association of Psychosocial Factors and Hospital Complications with Risk for Readmission After Trauma
- PMID: 33848832
- PMCID: PMC8222098
- DOI: 10.1016/j.jss.2021.02.031
Association of Psychosocial Factors and Hospital Complications with Risk for Readmission After Trauma
Abstract
Background: Unplanned hospital readmissions are associated with morbidity and high cost. Existing literature on readmission after trauma has focused on how injury characteristics are associated with readmission. We aimed to evaluate how psychosocial determinants of health and complications of hospitalization combined with injury characteristics affect risk of readmission after trauma.
Materials and methods: We conducted a retrospective cohort study of adult trauma admissions from July 2015 to September 2017 to Harborview Medical Center in Seattle, Washington. We assessed patient, injury, and hospitalization characteristics and estimated associations between risk factors and unplanned 30-d readmission using multivariable generalized linear Poisson regression models.
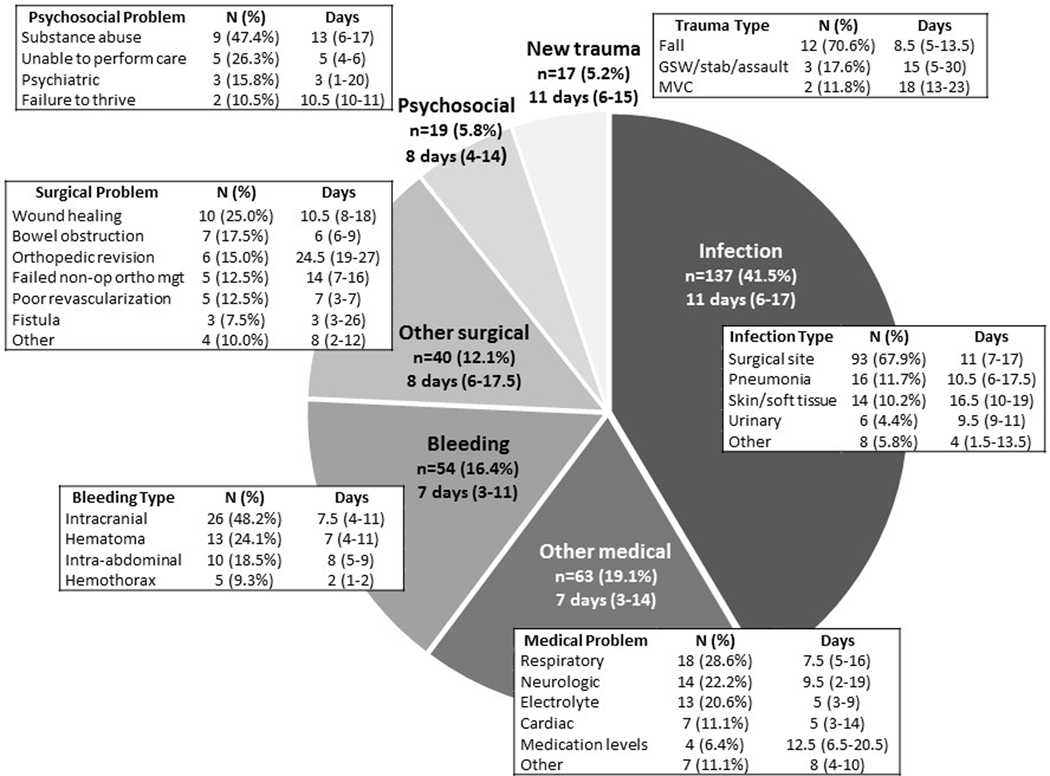
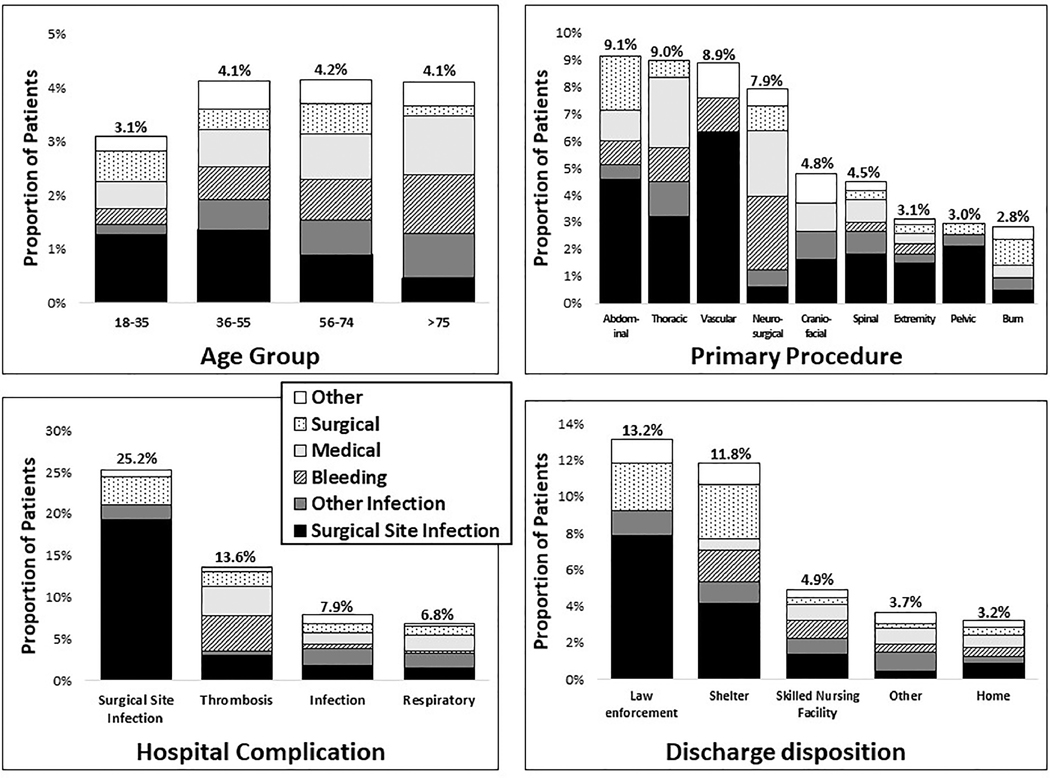
Results: Of 8916 discharged trauma patients, 330 (3.7%) had an unplanned 30-d readmission. Patients were most commonly readmitted with infection (41.5%). Independent risk factors for readmission among postoperative patients included public insurance (adjusted Relative Risk (aRR) 1.34, 95% CI 1.02-1.76), mental illness (aRR 1.39, 1.04-1.85), and chronic renal failure (aRR 2.17, 1.39-3.39); undergoing abdominal, thoracic, or neurosurgical procedures; experiencing an index hospitalization surgical site infection (aRR 4.74, 3.00-7.50), pulmonary embolism (aRR 3.38, 2.04-5.60), or unplanned ICU readmission (aRR 1.74, 1.16-2.62); shorter hospital stay (aRR 0.98/d, 0.97-0.99), and discharge to jail (aRR 4.68, 2.63-8.35) or a shelter (aRR 4.32, 2.58-7.21). Risk factors varied by reason for readmission. Injury severity, trauma mechanism, and body region were not independently associated with readmission risk.
Conclusions: Psychosocial factors and hospital complications were more strongly associated with readmission after trauma than injury characteristics. Improved social support and follow-up after discharge for high-risk patients may facilitate earlier identification of postdischarge complications.
Keywords: Patient readmission; risk factors; social determinants of health; trauma centers.
Copyright © 2021. Published by Elsevier Inc.
Conflict of interest statement
Figures
Similar articles
-
Impact of socio-economic status on unplanned readmission following injury: A multicenter cohort study.Injury. 2016 May;47(5):1083-90. doi: 10.1016/j.injury.2015.11.034. Epub 2015 Dec 12. Injury. 2016. PMID: 26746984
-
Trauma Center Outcomes After Transition From Level 2 to Level 1: A National Trauma Data Bank Analysis.J Surg Res. 2021 Aug;264:499-509. doi: 10.1016/j.jss.2021.03.021. Epub 2021 Apr 13. J Surg Res. 2021. PMID: 33857794
-
Early unplanned trauma readmissions in a safety net hospital are resource intensive but not due to resource limitations.J Trauma Acute Care Surg. 2017 Jul;83(1):135-138. doi: 10.1097/TA.0000000000001540. J Trauma Acute Care Surg. 2017. PMID: 28452893
-
The impact of frailty on posttraumatic outcomes in older trauma patients: A systematic review and meta-analysis.J Trauma Acute Care Surg. 2020 Apr;88(4):546-554. doi: 10.1097/TA.0000000000002583. J Trauma Acute Care Surg. 2020. PMID: 32205823
-
Reducing Readmission for Sepsis by Improving Risk Prediction Algorithms.Am J Crit Care. 2025 May 1;34(3):230-235. doi: 10.4037/ajcc2025455. Am J Crit Care. 2025. PMID: 40307178 Review.
Cited by
-
Status and Risk Factors in Patients Requiring Unplanned Intensive Care Unit Readmission Within 48 Hours: A Retrospective Propensity-Matched Study in China.Risk Manag Healthc Policy. 2023 Mar 11;16:383-391. doi: 10.2147/RMHP.S399829. eCollection 2023. Risk Manag Healthc Policy. 2023. PMID: 36936882 Free PMC article.
References
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418–1428. - PubMed
-
- Ashton CM, Del Junco DJ, Souchek J, et al. The association between the quality of inpatient care and early readmission: a meta-analysis of the evidence. Medical care. 1997;35(10):1044–1059. - PubMed
-
- Elixhauser A, Owens P. Reasons for Being Admitted to the Hospital through the Emergency Department, 2003: Statistical Brief #2. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Rockville (MD): Agency for Healthcare Research and Quality (US); 2006. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
