

School closures reduced social mixing of children during COVID-19 with implications for transmission risk and school reopening policies
- PMID: 33849340
- PMCID: PMC8086933
- DOI: 10.1098/rsif.2020.0970
School closures reduced social mixing of children during COVID-19 with implications for transmission risk and school reopening policies
Abstract
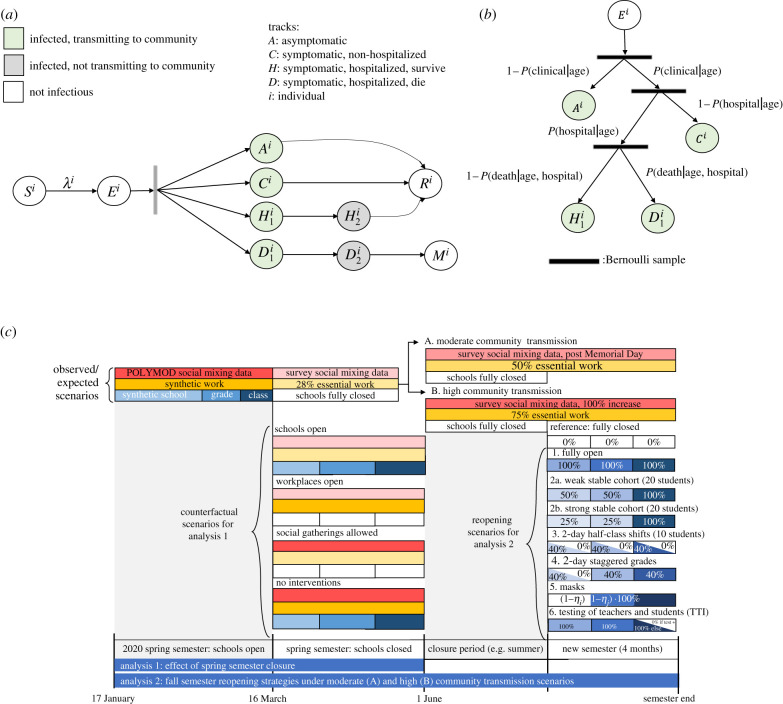
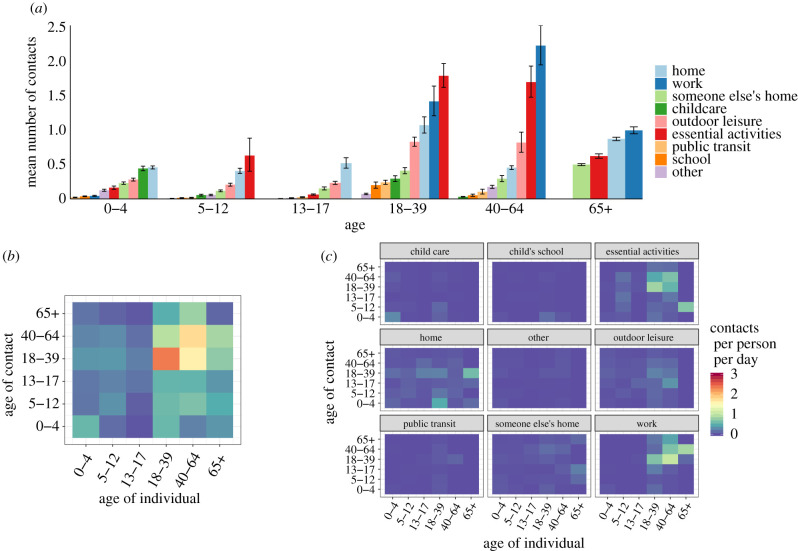
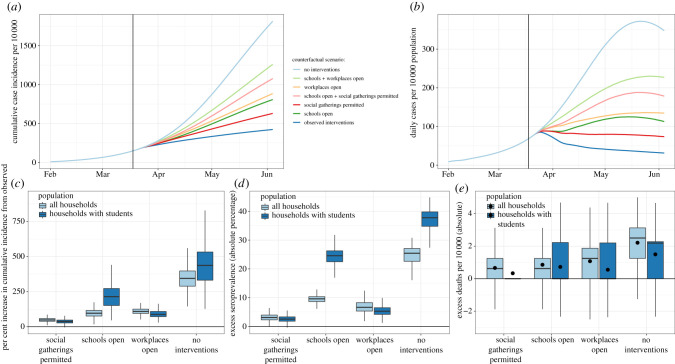
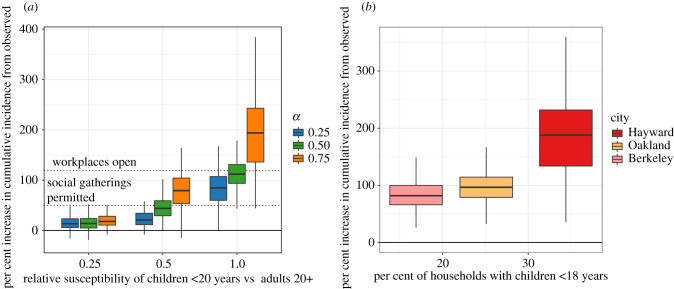
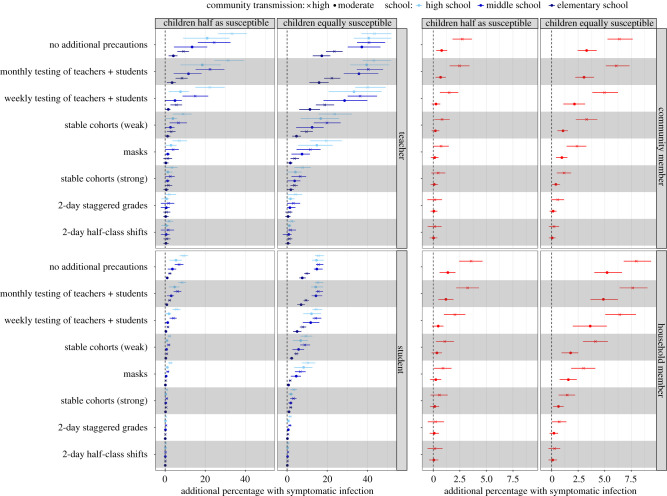
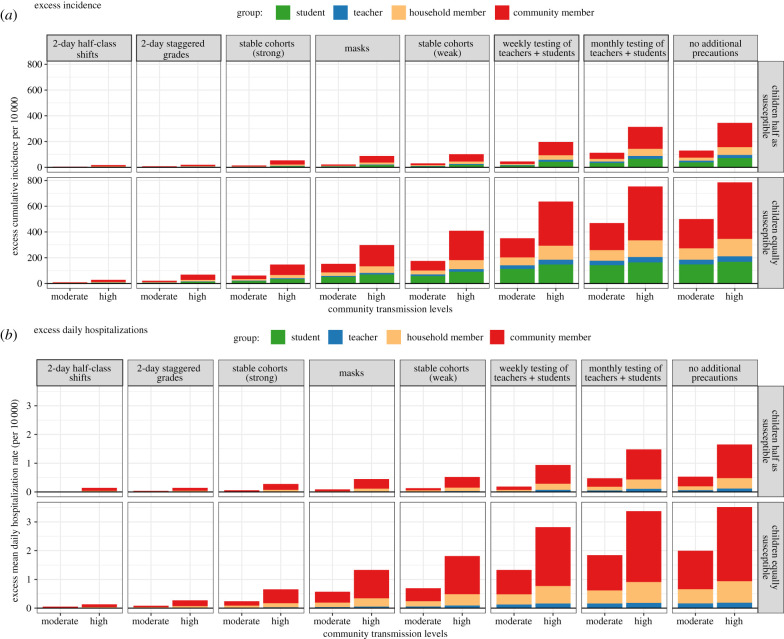
School closures may reduce the size of social networks among children, potentially limiting infectious disease transmission. To estimate the impact of K-12 closures and reopening policies on children's social interactions and COVID-19 incidence in California's Bay Area, we collected data on children's social contacts and assessed implications for transmission using an individual-based model. Elementary and Hispanic children had more contacts during closures than high school and non-Hispanic children, respectively. We estimated that spring 2020 closures of elementary schools averted 2167 cases in the Bay Area (95% CI: -985, 5572), fewer than middle (5884; 95% CI: 1478, 11.550), high school (8650; 95% CI: 3054, 15 940) and workplace (15 813; 95% CI: 9963, 22 617) closures. Under assumptions of moderate community transmission, we estimated that reopening for a four-month semester without any precautions will increase symptomatic illness among high school teachers (an additional 40.7% expected to experience symptomatic infection, 95% CI: 1.9, 61.1), middle school teachers (37.2%, 95% CI: 4.6, 58.1) and elementary school teachers (4.1%, 95% CI: -1.7, 12.0). However, we found that reopening policies for elementary schools that combine universal masking with classroom cohorts could result in few within-school transmissions, while high schools may require masking plus a staggered hybrid schedule. Stronger community interventions (e.g. remote work, social distancing) decreased the risk of within-school transmission across all measures studied, with the influence of community transmission minimized as the effectiveness of the within-school measures increased.
Keywords: COVID-19; SARS-CoV-2; children social networks; contact rate; school closures and reopening; transmission model.
Figures
Update of
-
The effect of school closures and reopening strategies on COVID-19 infection dynamics in the San Francisco Bay Area: a cross-sectional survey and modeling analysis.medRxiv [Preprint]. 2020 Aug 7:2020.08.06.20169797. doi: 10.1101/2020.08.06.20169797. medRxiv. 2020. Update in: J R Soc Interface. 2021 Apr;18(177):20200970. doi: 10.1098/rsif.2020.0970. PMID: 32793934 Free PMC article. Updated. Preprint.
References
-
- Yoshikawa H, Wuermli AJ, Britto PR, Dreyer B, Leckman JF, Lye SJ, Ponguta SJ, Richter LM, Stein A. 2020. Effects of the global coronavirus disease-2019 pandemic on early childhood development: short- and long-term risks and mitigating program and policy actions. J. Pediatr. 223, 188-193. ( 10.1016/j.jpeds.2020.05.020) - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous