

Implementation strategies to improve statin utilization in individuals with hypercholesterolemia: a systematic review and meta-analysis
- PMID: 33849601
- PMCID: PMC8045284
- DOI: 10.1186/s13012-021-01108-0
Implementation strategies to improve statin utilization in individuals with hypercholesterolemia: a systematic review and meta-analysis
Abstract
Background: Numerous implementation strategies to improve utilization of statins in patients with hypercholesterolemia have been utilized, with varying degrees of success. The aim of this systematic review is to determine the state of evidence of implementation strategies on the uptake of statins.
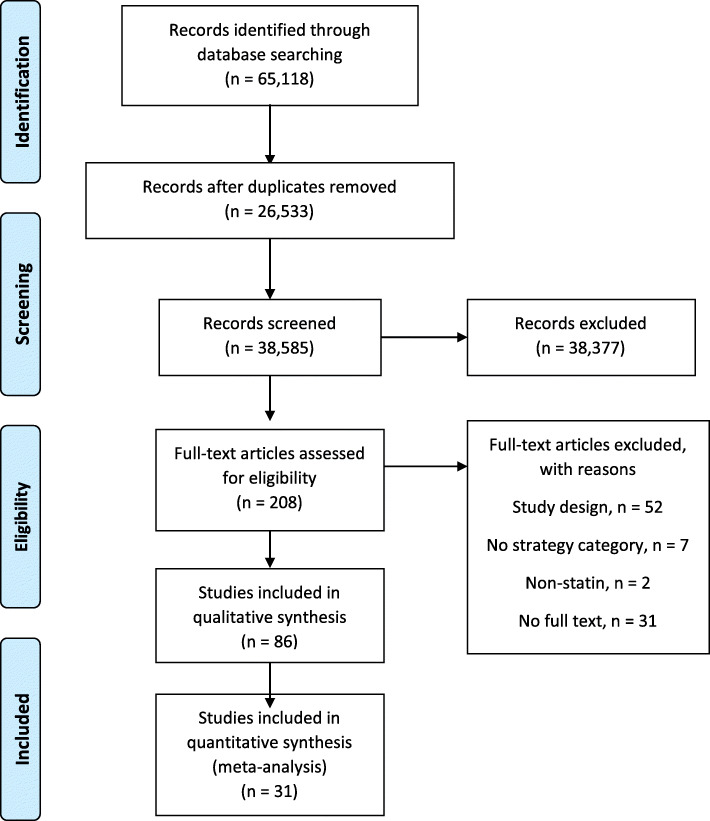
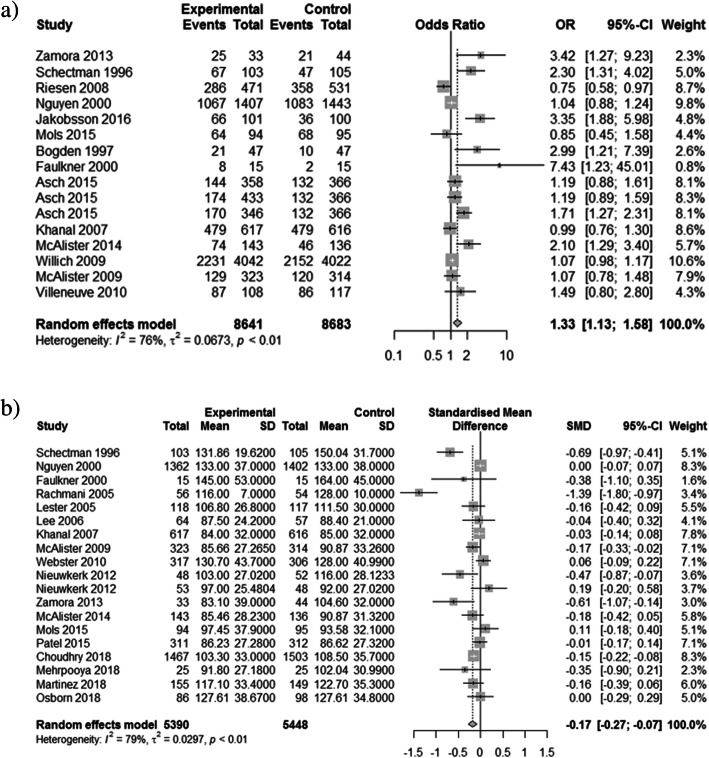
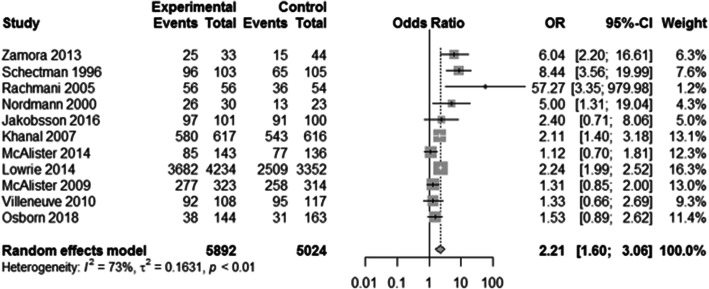
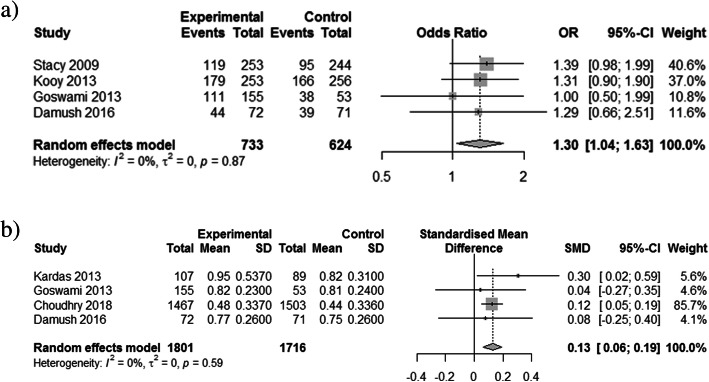
Methods and results: This systematic review identified and categorized implementation strategies, according to the Expert Recommendations for Implementing Change (ERIC) compilation, used in studies to improve statin use. We searched Ovid MEDLINE, Embase, Scopus, Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, and Clinicaltrials.gov from inception to October 2018. All included studies were reported in English and had at least one strategy to promote statin uptake that could be categorized using the ERIC compilation. Data extraction was completed independently, in duplicate, and disagreements were resolved by consensus. We extracted LDL-C (concentration and target achievement), statin prescribing, and statin adherence (percentage and target achievement). A total of 258 strategies were used across 86 trials. The median number of strategies used was 3 (SD 2.2, range 1-13). Implementation strategy descriptions often did not include key defining characteristics: temporality was reported in 59%, dose in 52%, affected outcome in 9%, and justification in 6%. Thirty-one trials reported at least 1 of the 3 outcomes of interest: significantly reduced LDL-C (standardized mean difference [SMD] - 0.17, 95% CI - 0.27 to - 0.07, p = 0.0006; odds ratio [OR] 1.33, 95% CI 1.13 to 1.58, p = 0.0008), increased rates of statin prescribing (OR 2.21, 95% CI 1.60 to 3.06, p < 0.0001), and improved statin adherence (SMD 0.13, 95% CI 0.06 to 0.19; p = 0.0002; OR 1.30, 95% CI 1.04 to 1.63, p = 0.023). The number of implementation strategies used per study positively influenced the efficacy outcomes.
Conclusion: Although studies demonstrated improved statin prescribing, statin adherence, and reduced LDL-C, no single strategy or group of strategies consistently improved outcomes.
Trial registration: PROSPERO CRD42018114952 .
Keywords: Hypercholesterolemia; Implementation strategies; Meta-analysis; Statin; Uptake.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Interventions for promoting habitual exercise in people living with and beyond cancer.Cochrane Database Syst Rev. 2018 Sep 19;9(9):CD010192. doi: 10.1002/14651858.CD010192.pub3. Cochrane Database Syst Rev. 2018. PMID: 30229557 Free PMC article.
-
Music interventions for improving psychological and physical outcomes in people with cancer.Cochrane Database Syst Rev. 2021 Oct 12;10(10):CD006911. doi: 10.1002/14651858.CD006911.pub4. Cochrane Database Syst Rev. 2021. PMID: 34637527 Free PMC article.
-
Sertindole for schizophrenia.Cochrane Database Syst Rev. 2005 Jul 20;2005(3):CD001715. doi: 10.1002/14651858.CD001715.pub2. Cochrane Database Syst Rev. 2005. PMID: 16034864 Free PMC article.
-
Eliciting adverse effects data from participants in clinical trials.Cochrane Database Syst Rev. 2018 Jan 16;1(1):MR000039. doi: 10.1002/14651858.MR000039.pub2. Cochrane Database Syst Rev. 2018. PMID: 29372930 Free PMC article.
-
Interventions for implementation of thromboprophylaxis in hospitalized patients at risk for venous thromboembolism.Cochrane Database Syst Rev. 2018 Apr 24;4(4):CD008201. doi: 10.1002/14651858.CD008201.pub3. Cochrane Database Syst Rev. 2018. PMID: 29687454 Free PMC article.
Cited by
-
LOGAN-CV: A Prospective Study of a Multifaceted Intervention Targeting United States Clinicians to Improve Guideline-Based Management of Lipid-Lowering Therapy.Adv Ther. 2024 Jan;41(1):451-463. doi: 10.1007/s12325-023-02716-6. Epub 2023 Nov 21. Adv Ther. 2024. PMID: 37989909 Free PMC article.
-
Impact of a Population Genomic Screening Program on Health Behaviors Related to Familial Hypercholesterolemia Risk Reduction.Circ Genom Precis Med. 2022 Oct;15(5):e003549. doi: 10.1161/CIRCGEN.121.003549. Epub 2022 Jul 12. Circ Genom Precis Med. 2022. PMID: 35862023 Free PMC article.
-
Application of the Expert Recommendations for Implementing Change (ERIC) compilation of strategies to health intervention implementation in low- and middle-income countries: a systematic review.Implement Sci. 2023 Oct 30;18(1):56. doi: 10.1186/s13012-023-01310-2. Implement Sci. 2023. PMID: 37904218 Free PMC article.
-
Learnings from Implementation Strategies to Improve Lipid Management.Curr Cardiol Rep. 2025 Jan 8;27(1):9. doi: 10.1007/s11886-024-02174-8. Curr Cardiol Rep. 2025. PMID: 39775142 Free PMC article. Review.
-
Intensity of and Adherence to Lipid-Lowering Therapy as Predictors of Major Adverse Cardiovascular Outcomes in Patients With Coronary Heart Disease.J Am Heart Assoc. 2022 Jul 19;11(14):e025813. doi: 10.1161/JAHA.122.025813. Epub 2022 Jul 5. J Am Heart Assoc. 2022. PMID: 35861825 Free PMC article.
References
-
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2019;139(25):e1082–e1143. - PMC - PubMed
-
- Akhabue E, Rittner SS, Carroll JE, et al. Implications of American College of Cardiology/American Heart Association (ACC/AHA) cholesterol guidelines on statin underutilization for prevention of cardiovascular disease in diabetes mellitus among several US networks of community health centers. J Am Heart Assoc. 2017;6(7):e005627. doi: 10.1161/JAHA.117.005627. - DOI - PMC - PubMed
-
- Bansilal S, Castellano JM, Garrido E, Wei HG, Freeman A, Spettell C, Garcia-Alonso F, Lizano I, Arnold RJG, Rajda J, Steinberg G, Fuster V. Assessing the impact of medication adherence on long-term cardiovascular outcomes. J Am Coll Cardiol. 2016;68(8):789–801. doi: 10.1016/j.jacc.2016.06.005. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
