

Death in hospital following ICU discharge: insights from the LUNG SAFE study
- PMID: 33849625
- PMCID: PMC8043098
- DOI: 10.1186/s13054-021-03465-0
Death in hospital following ICU discharge: insights from the LUNG SAFE study
Abstract
Background: To determine the frequency of, and factors associated with, death in hospital following ICU discharge to the ward.
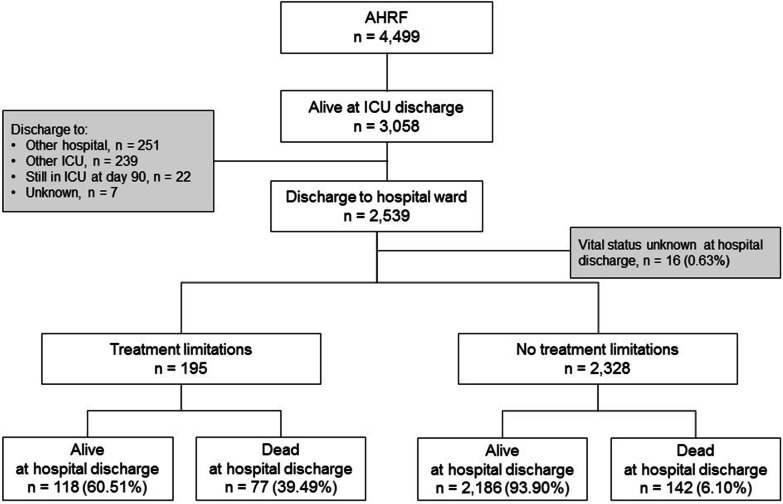
Methods: The Large observational study to UNderstand the Global impact of Severe Acute respiratory FailurE study was an international, multicenter, prospective cohort study of patients with severe respiratory failure, conducted across 459 ICUs from 50 countries globally. This study aimed to understand the frequency and factors associated with death in hospital in patients who survived their ICU stay. We examined outcomes in the subpopulation discharged with no limitations of life sustaining treatments ('treatment limitations'), and the subpopulations with treatment limitations.
Results: 2186 (94%) patients with no treatment limitations discharged from ICU survived, while 142 (6%) died in hospital. 118 (61%) of patients with treatment limitations survived while 77 (39%) patients died in hospital. Patients without treatment limitations that died in hospital after ICU discharge were older, more likely to have COPD, immunocompromise or chronic renal failure, less likely to have trauma as a risk factor for ARDS. Patients that died post ICU discharge were less likely to receive neuromuscular blockade, or to receive any adjunctive measure, and had a higher pre- ICU discharge non-pulmonary SOFA score. A similar pattern was seen in patients with treatment limitations that died in hospital following ICU discharge.
Conclusions: A significant proportion of patients die in hospital following discharge from ICU, with higher mortality in patients with limitations of life-sustaining treatments in place. Non-survivors had higher systemic illness severity scores at ICU discharge than survivors.
Trial registration: ClinicalTrials.gov NCT02010073 .
Keywords: Acute hypoxemic respiratory failure; Acute respiratory distress syndrome; Hospital survival; ICU discharge; LUNG SAFE.
Conflict of interest statement
Prof Laffey reports personal fees from consultancy for Baxter and Cala Medical, and funds to his institution from grants from Science Foundation Ireland, the Health Research Board and others. All other authors attest that they have no conflicts of interest in regard to the subject of this manuscript.
Figures



References
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, Gattinoni L, van Haren F, Larsson A, McAuley DF, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315(8):788–800. doi: 10.1001/jama.2016.0291. - DOI - PubMed
-
- Laffey JG, Madotto F, Bellani G, Pham T, Fan E, Brochard L, Amin P, Arabi Y, Bajwa EK, Bruhn A, et al. Geo-economic variations in epidemiology, patterns of care, and outcomes in patients with acute respiratory distress syndrome: insights from the LUNG SAFE prospective cohort study. Lancet Respir Med. 2017;5(8):627–638. doi: 10.1016/S2213-2600(17)30213-8. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
