

Validation of 18F-FDG PET/MRI and diffusion-weighted MRI for estimating the extent of peritoneal carcinomatosis in ovarian and endometrial cancer -a pilot study
- PMID: 33849649
- PMCID: PMC8042953
- DOI: 10.1186/s40644-021-00399-2
Validation of 18F-FDG PET/MRI and diffusion-weighted MRI for estimating the extent of peritoneal carcinomatosis in ovarian and endometrial cancer -a pilot study
Abstract
Background: The extent of peritoneal carcinomatosis is difficult to estimate preoperatively, but a valid measure would be important in identifying operable patients. The present study set out to validate the usefulness of integrated 18F-FDG PET/MRI, in comparison with diffusion-weighted MRI (DW-MRI), for estimation of the extent of peritoneal carcinomatosis in patients with gynaecological cancer.
Methods: Whole-body PET/MRI was performed on 34 patients with presumed carcinomatosis of gynaecological origin, all scheduled for surgery. Two radiologists evaluated the peritoneal cancer index (PCI) on PET/MRI and DW-MRI scans in consensus. The surgeon estimated PCI intraoperatively, which was used as the gold standard.
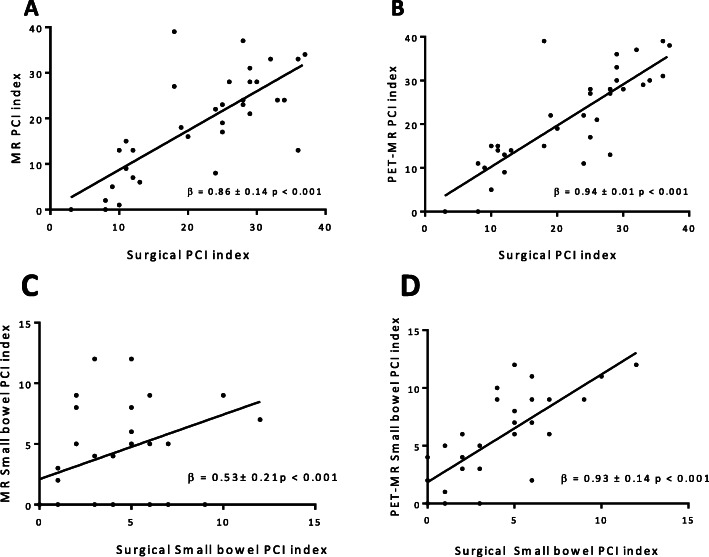
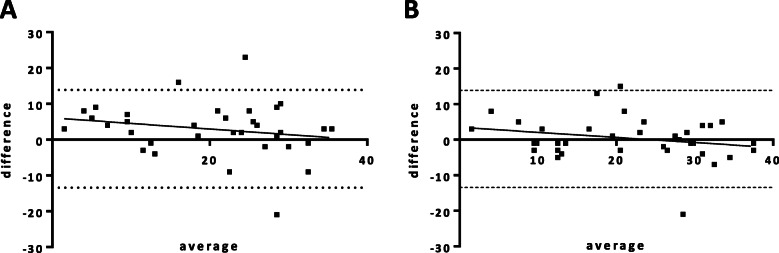
Results: Median total PCI for PET/MRI (21.5) was closer to surgical PCI (24.5) (p = 0.6), than DW-MRI (median PCI 20.0, p = 0.007). However, both methods were highly correlated with the surgical PCI (PET/MRI: β = 0.94 p < 0.01, DW-MRI: β = 0.86, p < 0.01). PET/MRI was more accurate (p = 0.3) than DW-MRI (p = 0.001) when evaluating patients at primary diagnosis but no difference was noted in patients treated with chemotherapy. PET/MRI was superior in evaluating high tumour burden in inoperable patients. In the small bowel regions, there was a tendency of higher sensitivity but lower specificity in PET/MRI compared to DW-MRI.
Conclusions: Our results suggest that FDG PET/MRI is superior to DW-MRI in estimating total spread of carcinomatosis in gynaecological cancer. Further, the greatest advantage of PET/MRI seems to be in patients at primary diagnosis and with high tumour burden, which suggest that it could be a useful tool when deciding about operability in gynaecological cancer.
Keywords: Carcinomatosis; DW-MRI; Ovarian cancer; PET/MRI; Peritoneal cancer index (PCI).
Conflict of interest statement
No competing interests have been identified.
Figures
Similar articles
-
Assessment of peritoneal metastases with DW-MRI, CT, and FDG PET/CT before cytoreductive surgery for advanced stage epithelial ovarian cancer.Eur J Surg Oncol. 2021 Aug;47(8):2134-2141. doi: 10.1016/j.ejso.2021.03.239. Epub 2021 Mar 16. Eur J Surg Oncol. 2021. PMID: 33812768
-
Positron emission tomography (PET) and magnetic resonance imaging (MRI) for assessing tumour resectability in advanced epithelial ovarian/fallopian tube/primary peritoneal cancer.Cochrane Database Syst Rev. 2018 Oct 8;10(10):CD012567. doi: 10.1002/14651858.CD012567.pub2. Cochrane Database Syst Rev. 2018. PMID: 30298516 Free PMC article.
-
Use of (18)F-FDG PET/CT in the preoperative evaluation of patients diagnosed with peritoneal carcinomatosis of ovarian origin, candidates to cytoreduction and hipec. A pending issue.Eur J Radiol. 2016 Oct;85(10):1824-1828. doi: 10.1016/j.ejrad.2016.08.006. Epub 2016 Aug 11. Eur J Radiol. 2016. PMID: 27666623
-
Whole-body diffusion-weighted MRI for operability assessment in patients with colorectal cancer and peritoneal metastases.Cancer Imaging. 2019 Jan 7;19(1):1. doi: 10.1186/s40644-018-0187-z. Cancer Imaging. 2019. PMID: 30616608 Free PMC article.
-
The emerging roles of functional imaging in ovarian cancer with peritoneal carcinomatosis.Clin Radiol. 2018 Jul;73(7):597-609. doi: 10.1016/j.crad.2018.03.009. Epub 2018 Apr 21. Clin Radiol. 2018. PMID: 29685803 Review.
Cited by
-
FDG-PET/MRI for the preoperative diagnosis and staging of peritoneal carcinomatosis: a prospective multireader pilot study.Abdom Radiol (NY). 2023 Dec;48(12):3634-3642. doi: 10.1007/s00261-022-03703-1. Epub 2022 Oct 29. Abdom Radiol (NY). 2023. PMID: 36308554
-
Endometrial Cancer: 2023 Revised FIGO Staging System and the Role of Imaging.Cancers (Basel). 2024 May 14;16(10):1869. doi: 10.3390/cancers16101869. Cancers (Basel). 2024. PMID: 38791948 Free PMC article. Review.
-
Prognostic Value of Pretreatment 18F-FDG-PET/CT Metabolic Parameters in Advanced High-Grade Serous Ovarian Cancer.Cancers (Basel). 2025 Feb 19;17(4):698. doi: 10.3390/cancers17040698. Cancers (Basel). 2025. PMID: 40002291 Free PMC article.
-
Concordance of Radiological, Laparoscopic and Laparotomic Scoring to Predict Complete Cytoreduction in Women with Advanced Ovarian Cancer.Cancers (Basel). 2023 Jan 13;15(2):500. doi: 10.3390/cancers15020500. Cancers (Basel). 2023. PMID: 36672451 Free PMC article.
-
Co-reactivity pattern of glucose metabolism and blood perfusion revealing DNA mismatch repair deficiency based on PET/DCE-MRI in endometrial cancer.Cancer Imaging. 2024 Nov 25;24(1):161. doi: 10.1186/s40644-024-00805-5. Cancer Imaging. 2024. PMID: 39582001 Free PMC article.
References
-
- Klint A, Tryggvadottir L, Bray F, Gislum M, Hakulinen T, Storm HH, et al. Trends in the survival of patients diagnosed with cancer in female genital organs in the Nordic countries 1964-2003 followed up to the end of 2006. Acta Oncol. 2010;49(5):632–643. doi: 10.3109/02841861003691945. - DOI - PubMed
-
- Socialstyrelsen. Cancerincidens i sverige 2013 [Available from: http://www.socialstyrelsen.se/Lists/Artikelkatalog/Attachments/19613/201.... Accessed 4 Dec 2020.
-
- Luyckx M, Leblanc E, Filleron T, Morice P, Darai E, Classe JM, Ferron G, Stoeckle E, Pomel C, Vinet B, Chereau E, Bergzoll C, Querleu D. Maximal cytoreduction in patients with FIGO stage IIIC to stage IV ovarian, fallopian, and peritoneal cancer in day-to-day practice: a retrospective French multicentric study. Int J Gynecol Cancer. 2012;22(8):1337–1343. doi: 10.1097/IGC.0b013e31826a3559. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
