

Afterload-related cardiac performance identifies cardiac impairment and associates with outcome in patients with septic shock: a retrospective cohort study
- PMID: 33849653
- PMCID: PMC8042871
- DOI: 10.1186/s40560-021-00549-5
Afterload-related cardiac performance identifies cardiac impairment and associates with outcome in patients with septic shock: a retrospective cohort study
Abstract
Background: Septic patients with cardiac impairment are with high mortality. Afterload-related cardiac performance (ACP), as a new tool for diagnosing septic cardiomyopathy (SCM), still needs to be evaluated for its impact on the prognosis for patients with septic shock.
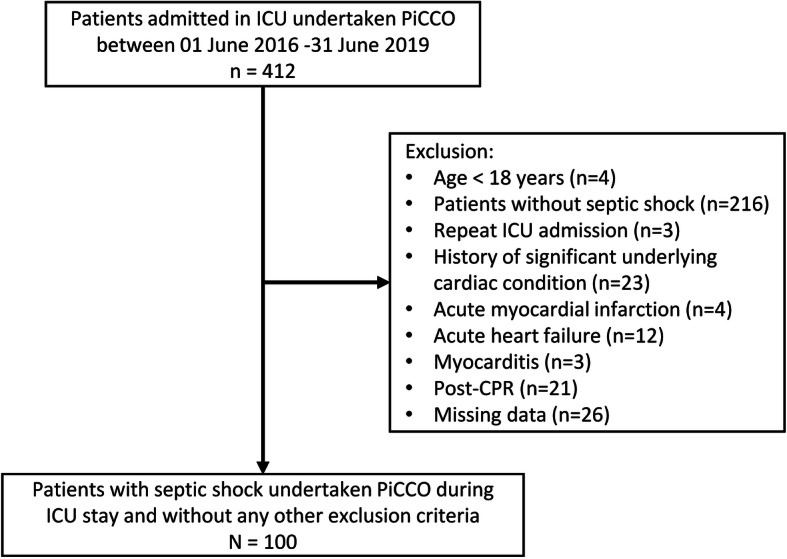
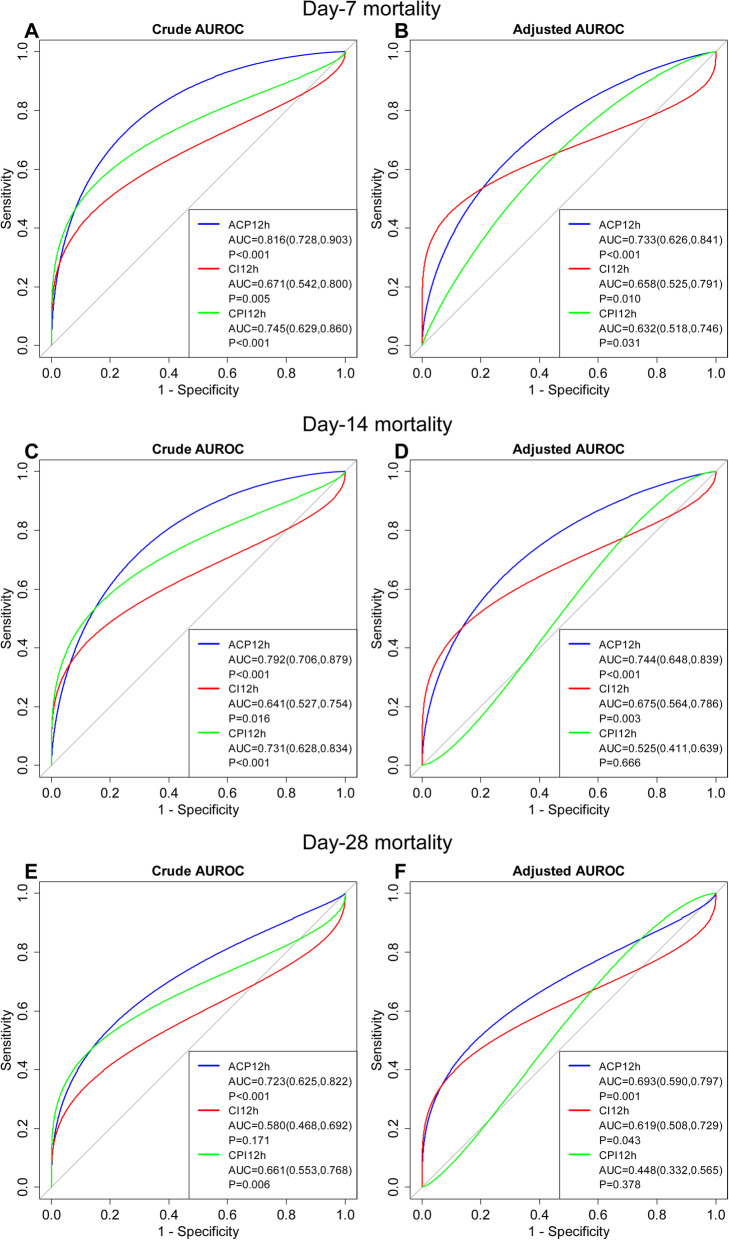
Methods: In this retrospective study, 100 patients with septic shock undertaken PiCCO monitoring were included. The ability of ACP, cardiac index (CI), and cardiac power index (CPI) to discriminate between survivors and non-survivors was tested by comparing the area under the receiver operating characteristic curve (AUROC) analysis. Cox proportional hazards regression analyses were performed to assess the associations of ACP with day-28 mortality. Curve estimation was used to describe the relationship between the hazard ratio (HR) of death and ACP.
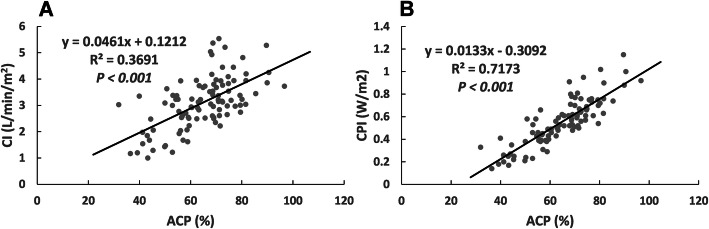
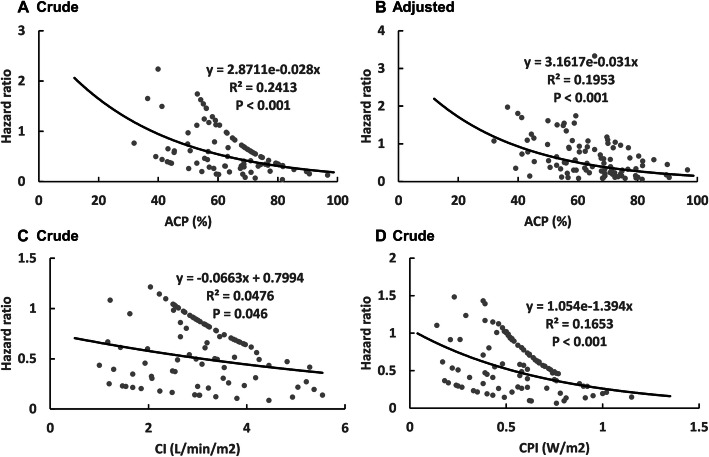
Results: ACP had a strong linear correlation with CI and CPI (P < 0.001). ACP demonstrated significantly greater discrimination for day-28 mortality than CI before adjusted [AUROC 0.723 (95% CI 0.625 to 0.822) vs. 0.580 (95% CI 0.468 to 0.692), P = 0.007] and CPI after adjusted [AUROC 0.693 (95% CI 0.590 to 0.797) vs. 0.448 (0.332 to 0.565), P < 0.001]. Compared with ACP > 68.78%, HR for ACP ≤ 68.78% was 3.55 (1.93 to 6.54) (P < 0.001). When adjusted with age, APACHE-II score, Vasoactive Inotropic Score, Lactate, CRRT, day-1 volume, fibrinogen and total bilirubin as possible confounders, and decrease ACP are still associated with increasing day-28 mortality (P < 0.05). An exponential relationship was observed between ACP12h and HR of day-28 death.
Conclusions: Our results suggested thatACP could improve mortality predictions when compared to CI and CPI. Decreased ACP was still an independent risk factor for increased day-28 mortality.
Keywords: Afterload-related cardiac performance; Cardiac index; Cardiac power index; Mortality; Septic cardiomyopathy.
Conflict of interest statement
The authors declare that they have no competing interests
Figures
References
-
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, Bellomo R, Bernard GR, Chiche JD, Coopersmith CM, Hotchkiss RS, Levy MM, Marshall JC, Martin GS, Opal SM, Rubenfeld GD, van der Poll T, Vincent JL, Angus DC. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) JAMA. 2016;315(8):801–810. doi: 10.1001/jama.2016.0287. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
