

Effectiveness of treatments for acute and subacute mechanical non-specific low back pain: a systematic review with network meta-analysis
- PMID: 33849907
- PMCID: PMC8685632
- DOI: 10.1136/bjsports-2020-103596
Effectiveness of treatments for acute and subacute mechanical non-specific low back pain: a systematic review with network meta-analysis
Abstract
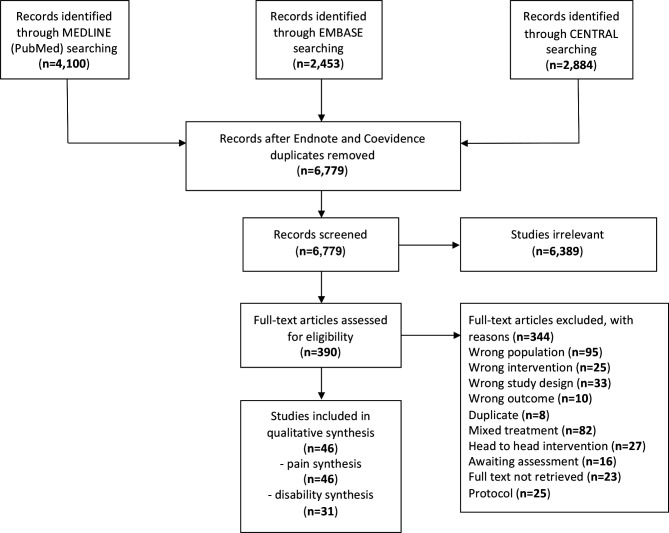
Objective: To assess the effectiveness of interventions for acute and subacute non-specific low back pain (NS-LBP) based on pain and disability outcomes.
Design: A systematic review of the literature with network meta-analysis.
Data sources: Medline, Embase and CENTRAL databases were searched from inception until 17 October 2020.
Eligibility criteria for selecting studies: Randomised clinical trials (RCTs) involving adults with NS-LBP who experienced pain for less than 6 weeks (acute) or between 6 and 12 weeks (subacute).
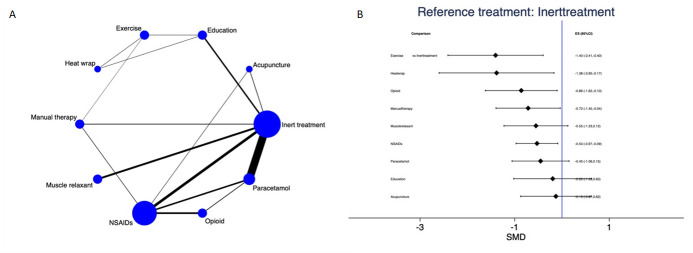
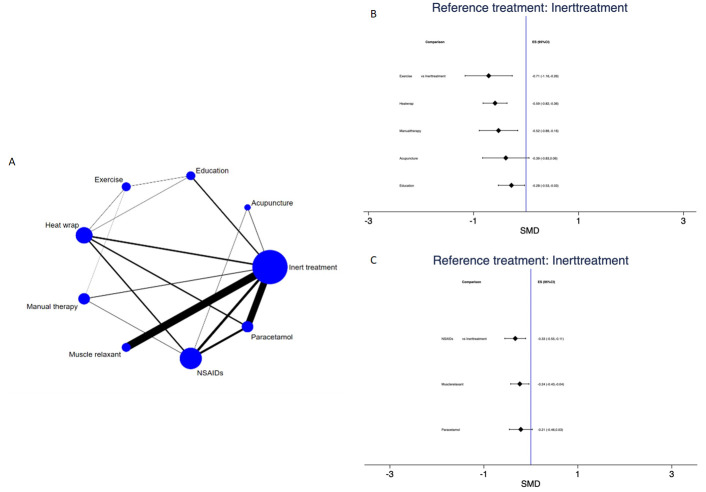
Results: Forty-six RCTs (n=8765) were included; risk of bias was low in 9 trials (19.6%), unclear in 20 (43.5%), and high in 17 (36.9%). At immediate-term follow-up, for pain decrease, the most efficacious treatments against an inert therapy were: exercise (standardised mean difference (SMD) -1.40; 95% confidence interval (CI) -2.41 to -0.40), heat wrap (SMD -1.38; 95% CI -2.60 to -0.17), opioids (SMD -0.86; 95% CI -1.62 to -0.10), manual therapy (SMD -0.72; 95% CI -1.40 to -0.04) and non-steroidal anti-inflammatory drugs (NSAIDs) (SMD -0.53; 95% CI -0.97 to -0.09). Similar findings were confirmed for disability reduction in non-pharmacological and pharmacological networks, including muscle relaxants (SMD -0.24; 95% CI -0.43 to -0.04). Mild or moderate adverse events were reported in the opioids (65.7%), NSAIDs (54.3%) and steroids (46.9%) trial arms.
Conclusion: With uncertainty of evidence, NS-LBP should be managed with non-pharmacological treatments which seem to mitigate pain and disability at immediate-term. Among pharmacological interventions, NSAIDs and muscle relaxants appear to offer the best harm-benefit balance.
Keywords: disability; evidence based review; lower back; pharmacology; rehabilitation.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Institute for health metrics and evaluation, 2018. Available: http://www.healthdata.org/data-visualization/gbd-compare
-
- Casazza BA. Diagnosis and treatment of acute low back pain. Am Fam Physician 2012;85:343–50. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous