

Non-functional pancreatic neuroendocrine tumours: ATRX/DAXX and alternative lengthening of telomeres (ALT) are prognostically independent from ARX/PDX1 expression and tumour size
- PMID: 33849943
- PMCID: PMC8511349
- DOI: 10.1136/gutjnl-2020-322595
Non-functional pancreatic neuroendocrine tumours: ATRX/DAXX and alternative lengthening of telomeres (ALT) are prognostically independent from ARX/PDX1 expression and tumour size
Abstract
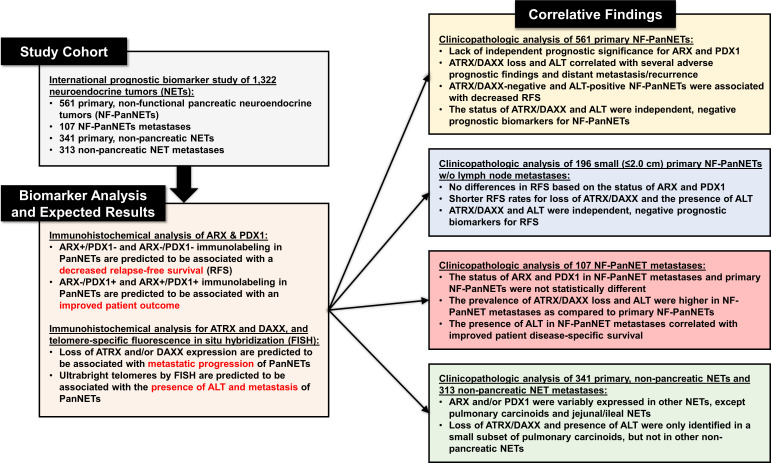
Objective: Recent studies have found aristaless-related homeobox gene (ARX)/pancreatic and duodenal homeobox 1 (PDX1), alpha-thalassemia/mental retardation X-linked (ATRX)/death domain-associated protein (DAXX) and alternative lengthening of telomeres (ALT) to be promising prognostic biomarkers for non-functional pancreatic neuroendocrine tumours (NF-PanNETs). However, they have not been comprehensively evaluated, especially among small NF-PanNETs (≤2.0 cm). Moreover, their status in neuroendocrine tumours (NETs) from other sites remains unknown.
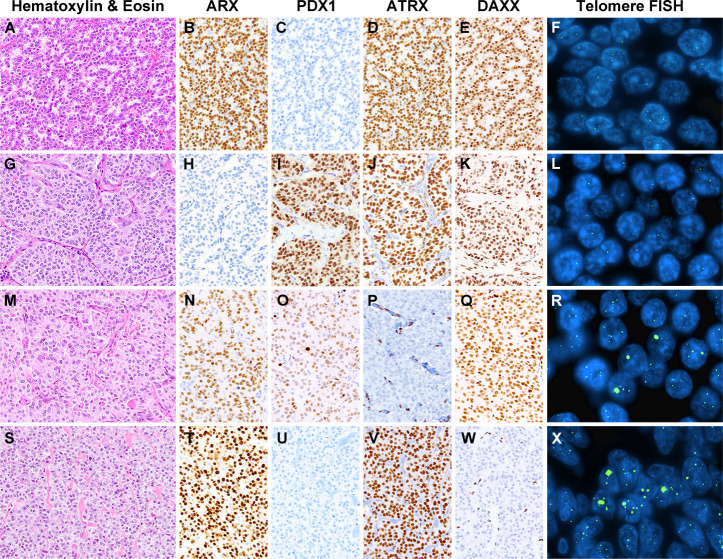
Design: An international cohort of 1322 NETs was evaluated by immunolabelling for ARX/PDX1 and ATRX/DAXX, and telomere-specific fluorescence in situ hybridisation for ALT. This cohort included 561 primary NF-PanNETs, 107 NF-PanNET metastases and 654 primary, non-pancreatic non-functional NETs and NET metastases. The results were correlated with numerous clinicopathological features including relapse-free survival (RFS).
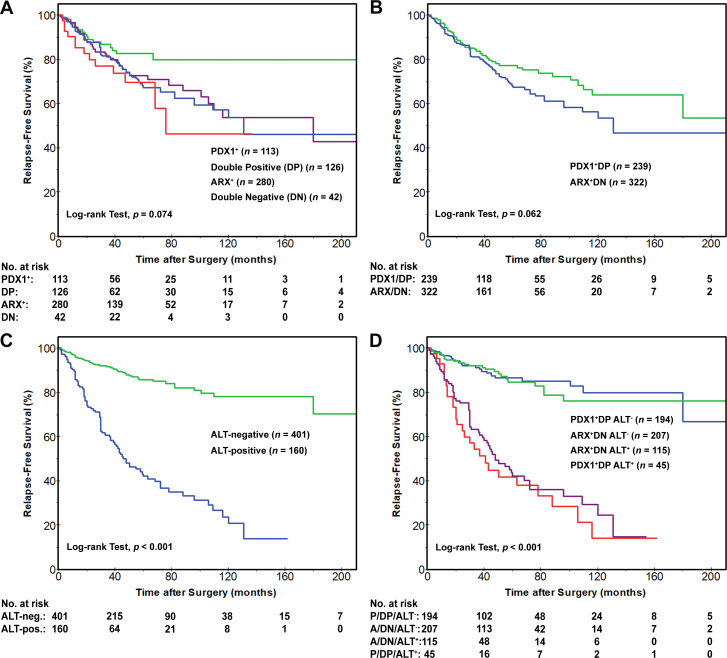
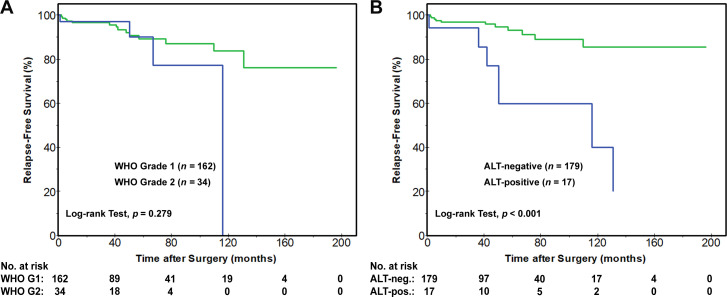
Results: ATRX/DAXX loss and ALT were associated with several adverse prognostic findings and distant metastasis/recurrence (p<0.001). The 5-year RFS rates for patients with ATRX/DAXX-negative and ALT-positive NF-PanNETs were 40% and 42% as compared with 85% and 86% for wild-type NF-PanNETs (p<0.001 and p<0.001). Shorter 5-year RFS rates for ≤2.0 cm NF-PanNETs patients were also seen with ATRX/DAXX loss (65% vs 92%, p=0.003) and ALT (60% vs 93%, p<0.001). By multivariate analysis, ATRX/DAXX and ALT status were independent prognostic factors for RFS. Conversely, classifying NF-PanNETs by ARX/PDX1 expression did not independently correlate with RFS. Except for 4% of pulmonary carcinoids, ATRX/DAXX loss and ALT were only identified in primary (25% and 29%) and NF-PanNET metastases (62% and 71%).
Conclusions: ATRX/DAXX and ALT should be considered in the prognostic evaluation of NF-PanNETs including ≤2.0 cm tumours, and are highly specific for pancreatic origin among NET metastases of unknown primary.
Keywords: neuroendocrine tumors; pancreatic endocrine tumour; pancreatic islet cell; pancreatic pathology; pancreatic surgery.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Prognostic value of DAXX/ATRX loss of expression and ALT activation in PanNETs: is it time for clinical implementation?Gut. 2022 May;71(5):847-848. doi: 10.1136/gutjnl-2021-324664. Epub 2021 May 11. Gut. 2022. PMID: 33975869 Free PMC article. No abstract available.
References
-
- Howlader N, Noone AM, Krapcho M. Seer cancer statistics review, 1975-2017. Bethesda, MD: National Cancer Institute, 2019.
-
- Network NCC . Neuroendocrine and adrenal tumors (version 1.2019), 2019.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials