

Comparison of the Quantitative DiaSorin Liaison Antigen Test to Reverse Transcription-PCR for the Diagnosis of COVID-19 in Symptomatic and Asymptomatic Outpatients
- PMID: 33849953
- PMCID: PMC8218764
- DOI: 10.1128/JCM.00374-21
Comparison of the Quantitative DiaSorin Liaison Antigen Test to Reverse Transcription-PCR for the Diagnosis of COVID-19 in Symptomatic and Asymptomatic Outpatients
Abstract
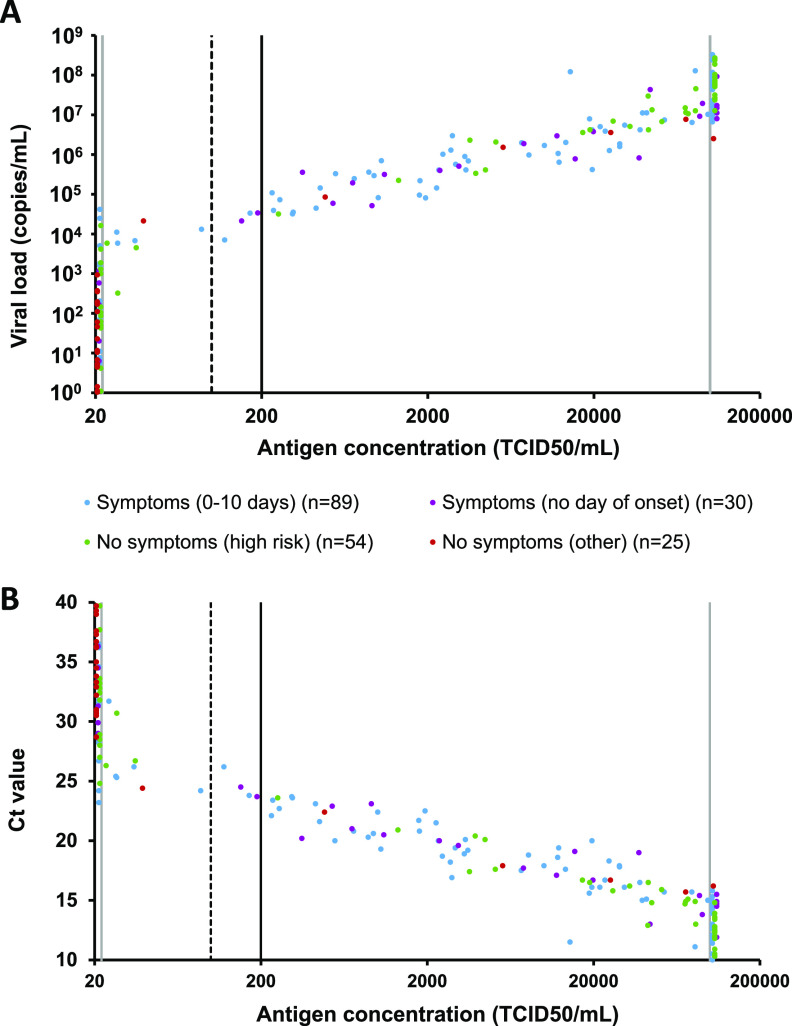
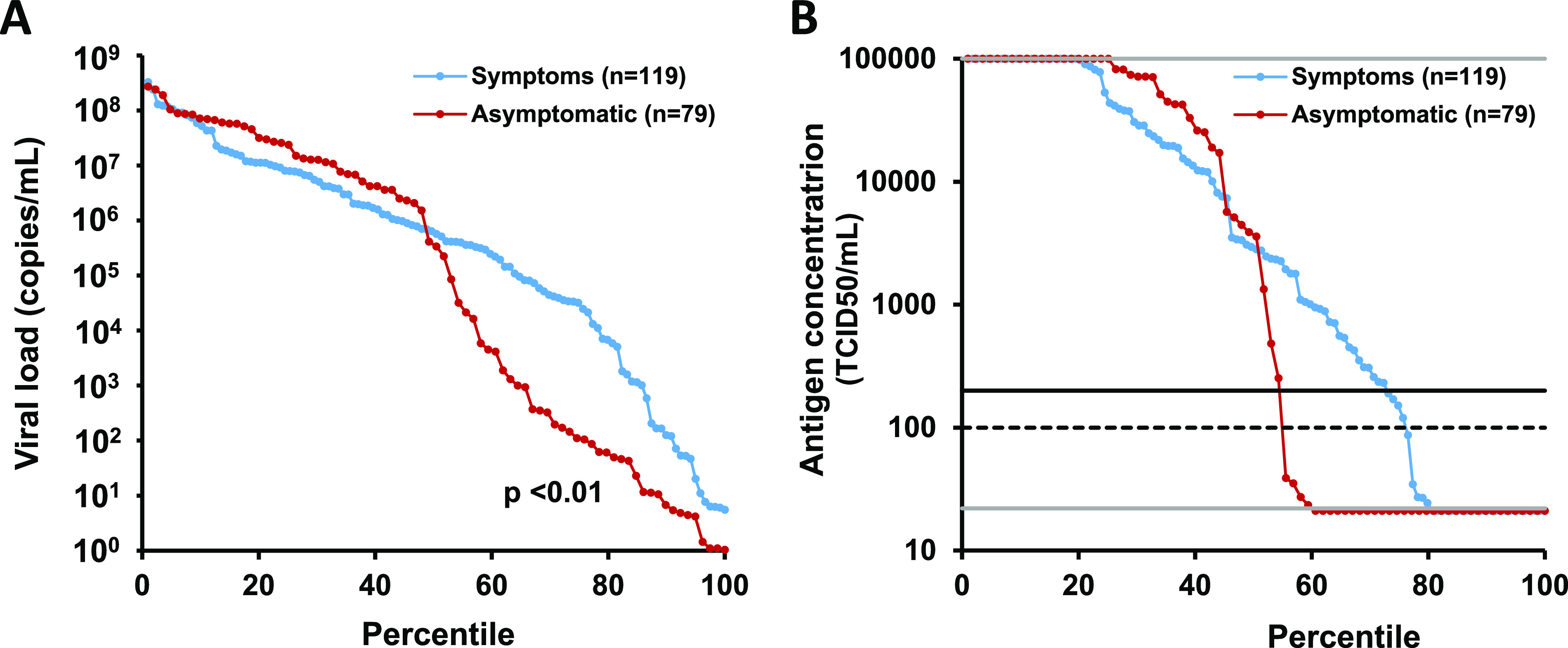
We evaluated the quantitative DiaSorin Liaison severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) antigen test in symptomatic and asymptomatic individuals consulting their general practitioners (GPs) during a period of stable intense virus circulation (213/100,000 habitants per day). Leftover reverse transcription-PCR (RT-PCR) positive (n = 204) and negative (n = 210) nasopharyngeal samples were randomly selected among fresh routine samples collected from patients consulting their GPs. Samples were tested on Liaison XL according to the manufacturer's instructions. Equivocal results were considered negative. The overall sensitivity and specificity of the Liaison antigen test compared to RT-PCR were 65.7% (95% confidence interval [CI], 58.9% to 71.9%) and 100% (CI, 97.8% to 100%). Sensitivity in samples with viral loads of ≥105, ≥104, and ≥103 copies/ml were 100% (CI, 96.3% to 100.0%), 96.5% (CI, 91.8% to 98.7%), and 87.4% (CI, 81.3% to 91.5%), respectively. All samples with ≤103 copies/ml were antigen negative. The ratio of antigen concentration to viral load in samples with ≥103 copies/ml was comparable in symptomatic and asymptomatic individuals (P = 0.58). The proportion of RT-PCR-positive participants with a high viral load (≥105 copies/ml) was not significantly higher in symptomatic than in asymptomatic participants (63.9% [CI, 54.9% to 72.0%] versus 51.9% [CI, 41.1% to 62.6%]; P = 0.11), but the proportion of participants with a low viral load (<103 copies/ml) was significantly higher in asymptomatic than in symptomatic RT-PCR-positive participants (35.4% [CI, 25.8% to 46.4%] versus 14.3% [CI, 9.0% to 21.8%]; P < 0.01). Sensitivity and specificity in samples with a viral load of ≥104 copies/ml were 96.5% and 100%. The correlation of antigen concentration with viral load was comparable in symptomatic and asymptomatic individuals.
Keywords: COVID-19 testing; SARS-CoV-2; ambulatory care; antigen; diagnosis; sensitivity and specificity.
Figures

References
-
- World Health Organization. 2020. SARS-CoV-2 antigen-detecting rapid diagnostic tests: an implementation guide. https://www.who.int/publications/i/item/9789240017740
-
- Young S, Taylor SN, Cammarata CL, Roger-Dalbert C, Montano A, Griego-Fullbright C, Burgard C, Fernandez C, Eckert K, Andrews JC, Ren H, Allen J, Ackerman R, Cooper CK. 2020. Clinical evaluation of BD VeritorTM SARS-CoV-2 point-of-care test performance compared to PCR-based testing and versus the Sofia 2 SARS antigen point-of-care test. J Clin Microbiol 17:e02338-20. 10.1128/JCM.02338-20. - DOI - PMC - PubMed
-
- Atkeson A, Droste M, Stock JH, Mina MJ. 2020. Economic benefits of COVID-19 screening tests. medRxiv 10.1101/2020.10.22.20217984. - DOI
-
- Van Elslande J, Houben E, Depypere M, Brackenier A, Desmet S, André E, Van Ranst M, Lagrou K, Vermeersch P. 2020. Diagnostic performance of seven rapid IgG/IgM antibody tests and the Euroimmun IgA/IgG ELISA in COVID-19 patients. Clin Microbiol Infect 26:1082–1087. 10.1016/j.cmi.2020.05.023. - DOI - PMC - PubMed
-
- Dinnes J, Deeks JJ, Adriano A, Berhane S, Davenport C, Dittrich S, Emperador D, Takwoingi Y, Cunningham J, Beese S, Dretzke J, Ferrante di Ruffano L, Harris IM, Price MJ, Taylor-Phillips S, Hooft L, Leeflang MM, Spijker R, Van den Bruel A, Cochrane COIVD-19 Diagnostic Test Accuracy Group . 2020. Rapid, point-of-care antigen and molecular-based tests for diagnosis of SARS-CoV-2 infection. Cochrane Database Syst Rev 26:CD013705. 10.1002/14651858.CD013705. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
