

Obstetric and perinatal health outcomes after pertussis vaccination during pregnancy in Ontario, Canada: a retrospective cohort study
- PMID: 33849984
- PMCID: PMC8084546
- DOI: 10.9778/cmajo.20200239
Obstetric and perinatal health outcomes after pertussis vaccination during pregnancy in Ontario, Canada: a retrospective cohort study
Abstract
Background: In February 2018, Canada's National Advisory Committee on Immunization recommended maternal vaccination with tetanus-diphtheria-acellular pertussis (Tdap) vaccine during pregnancy to prevent severe pertussis infection in young infants. This study assessed the relation between maternal Tdap vaccination and obstetric and perinatal outcomes in Ontario.
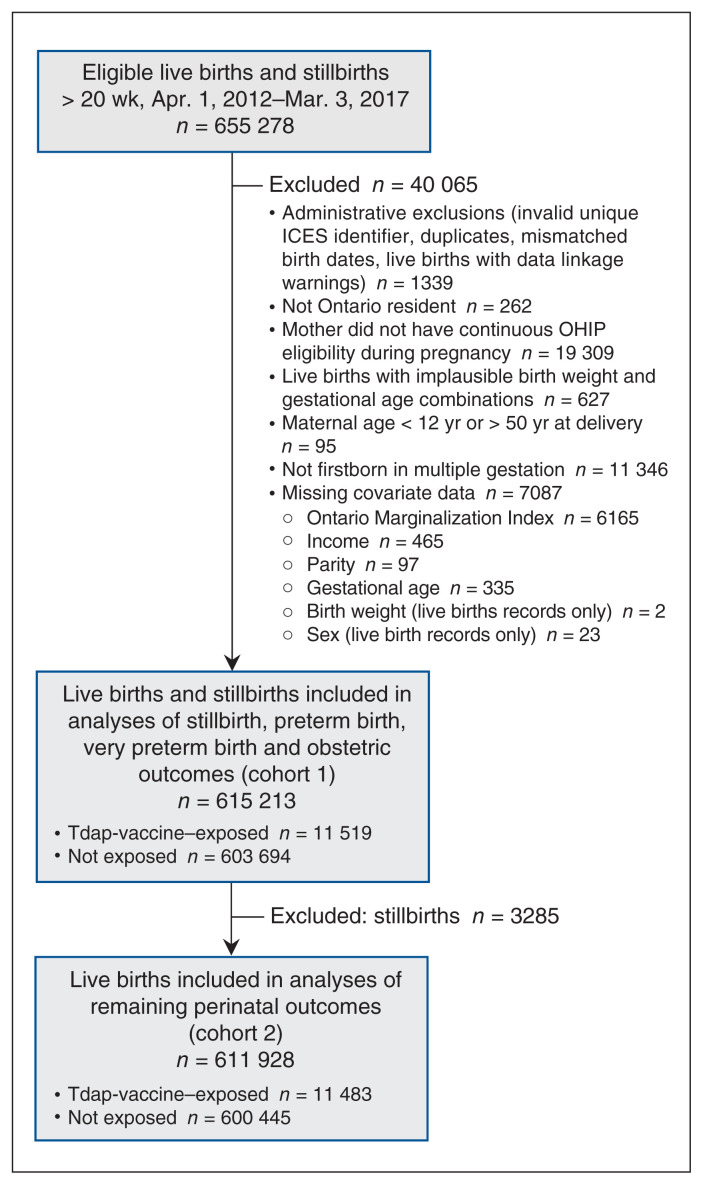
Methods: We performed a population-based cohort study of all births from April 2012 to March 2017 using multiple linked health administrative databases. We used Cox regression with a time-dependent exposure variable to estimate adjusted hazard ratios (HRs) for preterm birth (< 37 wk), very preterm birth (< 32 wk) and stillbirth. We assessed remaining outcomes (gestational hypertension, chorioamnionitis, postpartum hemorrhage, severe postpartum hemorrhage, being small for gestational age, neonatal intensive care unit stay > 24 h, composite neonatal morbidity) using log-binomial regression to generate adjusted risk ratios (RRs). We adjusted estimates for potential confounding using propensity score weighting.
Results: Of 615 213 infants (live births and stillbirths), 11 519 were exposed to Tdap vaccination in utero. There was no increased risk for preterm birth (adjusted HR 0.98, 95% confidence interval [CI] 0.91-1.06), very preterm birth (adjusted HR 1.10, 95% CI 0.86-1.41), stillbirth (adjusted HR 1.15, 95% CI 0.82-1.60) or being small for gestational age (adjusted RR 0.96, 95% CI 0.90-1.02). The risks of a neonatal intensive care unit stay exceeding 24 hours (adjusted RR 0.82, 95% CI 0.76-0.88) and neonatal morbidity (adjusted RR 0.81, 95% CI 0.75-0.87) were decreased. There was no association with chorioamnionitis (adjusted RR 1.17, 95% CI 0.99-1.39), postpartum hemorrhage (adjusted RR 1.01, 95% CI 0.91-1.13) or severe postpartum hemorrhage (adjusted RR 0.79, 95% CI 0.55-1.13), but we observed a reduced risk of gestational hypertension (adjusted RR 0.87, 95% CI 0.78-0.96).
Interpretation: Our results complement evidence that maternal Tdap vaccination is not associated with adverse outcomes in mothers or infants. Ongoing evaluation in Canada is needed as maternal Tdap vaccination coverage increases in coming years.
© 2021 Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: Scott Halperin has received research grants and contracts from and has served on ad hoc advisory boards for GlaxoSmithKline and Sanofi Pasteur, manufacturers of tetanus–diphtheria– acellular pertussis vaccines, unrelated to this study. Manish Sadarangani is supported by salary awards from the BC Children’s Hospital Foundation, the Canadian Child Health Clinician Scientist Program and the Michael Smith Foundation for Health Research. He has been an investigator on projects funded by Pfizer, Merck, Seqirus, VBI Vaccines, GlaxoSmithKline and Sanofi Pasteur; all funds have been paid to his institute, and he has not received any personal payments. Kumanan Wilson is married to an employee of CMAJ, who was not involved with the editorial decision-making process for this article. No other competing interests were declared.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous