

Associations between frontal lobe structure, parent-reported obstructive sleep disordered breathing and childhood behavior in the ABCD dataset
- PMID: 33850154
- PMCID: PMC8044120
- DOI: 10.1038/s41467-021-22534-0
Associations between frontal lobe structure, parent-reported obstructive sleep disordered breathing and childhood behavior in the ABCD dataset
Abstract
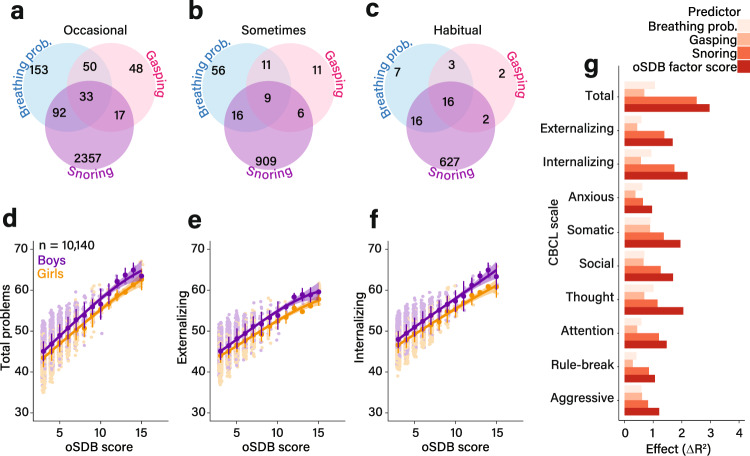
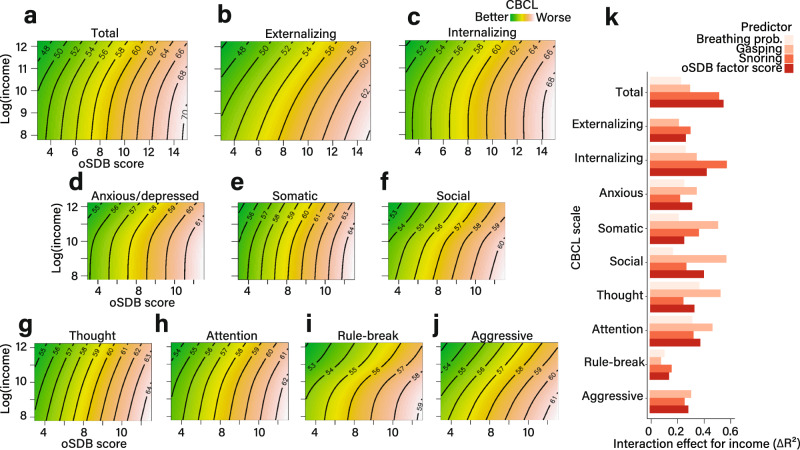
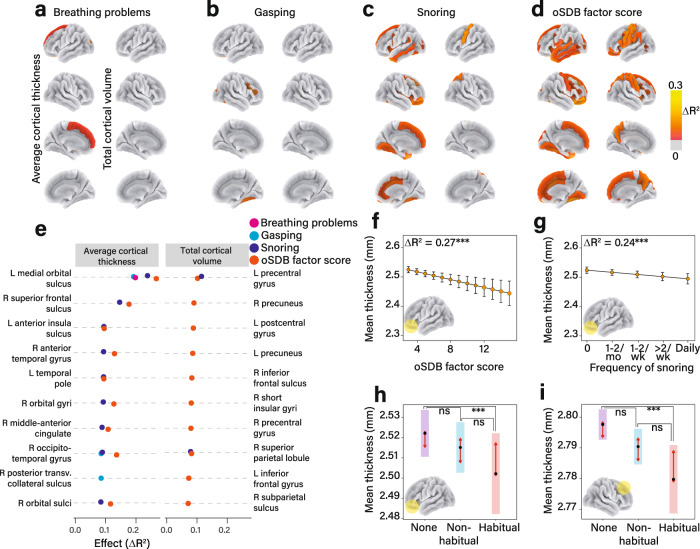
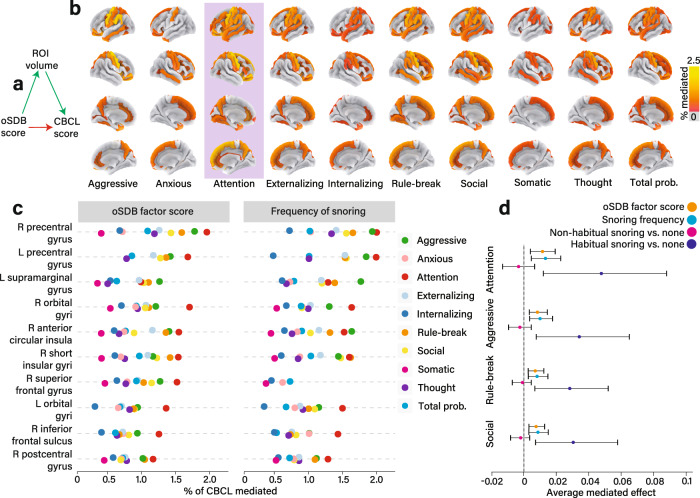
Parents frequently report behavioral problems among children who snore. Our understanding of the relationship between symptoms of obstructive sleep disordered breathing (oSDB) and childhood behavioral problems associated with brain structural alterations is limited. Here, we examine the associations between oSDB symptoms, behavioral measures such as inattention, and brain morphometry in the Adolescent Brain Cognitive Development (ABCD) study comprising 10,140 preadolescents. We observe that parent-reported symptoms of oSDB are associated with composite and domain-specific problem behaviors measured by parent responses to the Child Behavior Checklist. Alterations of brain structure demonstrating the strongest negative associations with oSDB symptoms are within the frontal lobe. The relationships between oSDB symptoms and behavioral measures are mediated by significantly smaller volumes of multiple frontal lobe regions. These results provide population-level evidence for an association between regional structural alterations in cortical gray matter and problem behaviors reported in children with oSDB.
Conflict of interest statement
Amal Isaiah has patents (pending or granted) related to the diagnosis and treatment of sleep apnea in adults using ultrasound. These have been licensed by the University of Maryland, Baltimore. They are not discussed in the current manuscript. All others declare no competing interests.
Figures
Comment in
-
Neurocognition, Behavior, Socioeconomic, and Health Outcomes of Pediatric Obstructive Sleep Apnea.Am J Respir Crit Care Med. 2023 Apr 1;207(7):936-938. doi: 10.1164/rccm.202201-0051RR. Am J Respir Crit Care Med. 2023. PMID: 36689760 No abstract available.
References
Publication types
MeSH terms
Grants and funding
- U01 DA041174/DA/NIDA NIH HHS/United States
- U01 DA041048/DA/NIDA NIH HHS/United States
- U01 DA041156/DA/NIDA NIH HHS/United States
- U01 DA041093/DA/NIDA NIH HHS/United States
- U01 DA041106/DA/NIDA NIH HHS/United States
- U01 DA050989/DA/NIDA NIH HHS/United States
- U01 DA041089/DA/NIDA NIH HHS/United States
- U01 DA050988/DA/NIDA NIH HHS/United States
- U01 DA041028/DA/NIDA NIH HHS/United States
- U01 DA041134/DA/NIDA NIH HHS/United States
- U24 DA041147/DA/NIDA NIH HHS/United States
- U01 DA050987/DA/NIDA NIH HHS/United States
- P50 DA046346/DA/NIDA NIH HHS/United States
- U01 DA041022/DA/NIDA NIH HHS/United States
- U01 DA041025/DA/NIDA NIH HHS/United States
- U01 DA051037/DA/NIDA NIH HHS/United States
- U01 DA051016/DA/NIDA NIH HHS/United States
- U01 DA041148/DA/NIDA NIH HHS/United States
- U24 DA041123/DA/NIDA NIH HHS/United States
- U01 DA041117/DA/NIDA NIH HHS/United States
- U01 DA041120/DA/NIDA NIH HHS/United States
- U01 DA051039/DA/NIDA NIH HHS/United States
- U01 DA051018/DA/NIDA NIH HHS/United States
- U01 DA051038/DA/NIDA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
