

MRI of the Achilles tendon-A comprehensive pictorial review. Part one
- PMID: 33850971
- PMCID: PMC8039565
- DOI: 10.1016/j.ejro.2021.100342
MRI of the Achilles tendon-A comprehensive pictorial review. Part one
Abstract
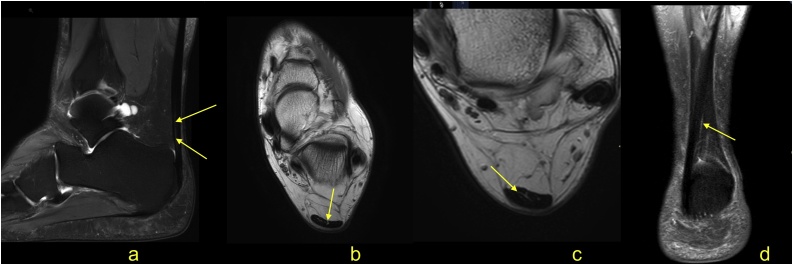
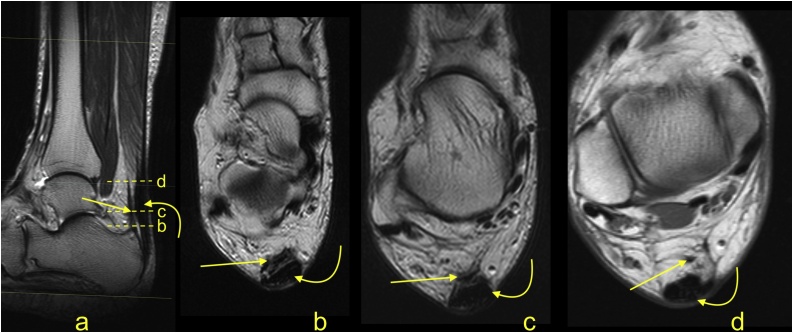
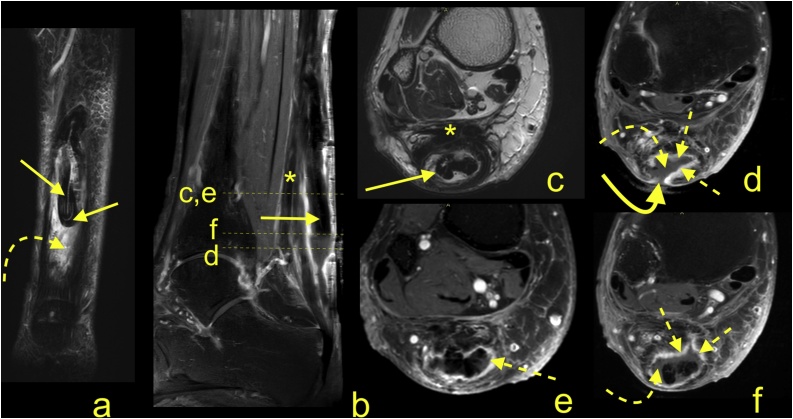
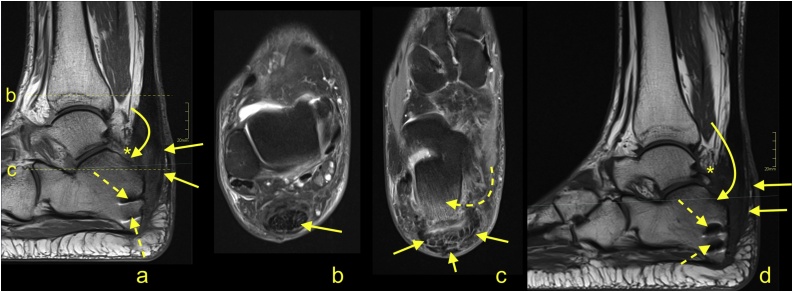
The normal Achilles tendon is composed of twisted subtendons separated by thin high signal septae, which are a potential pitfall on MRI because they mimic a tendon tear. Tendinopathy and full thickness tears may be assessed effectively both on MRI and ultrasound. MRI is superior to ultrasound in detection of partial tears and for postoperative assessment. The use of fat suppression sequences allows the ability to detect focal lesions. Sagittal and coronal sections are useful for assessing the distance between stumps of a ruptured tendon. Sequences with contrast are indicated in postoperative investigations and suspicion of infection, arthritis or tumor. MRI may reveal inflammatory changes with minor symptoms long before the clinical manifestations of seronegative spondyloarthropathy. The most common non-traumatic focal lesion of the Achilles tendon is Achilles tendon xanthoma, which is manifested by intermediate or slightly higher signal on T1- and T2-weighted images compared to that in the normal Achilles tendon. Other tumors of the Achilles tendon are very rare, whereas the involvement of the tendon from tumor in adjacent structures is more frequent. The novel MRI sequences may help to detect disorders of the Achilles tendon more specifically before clinical manifestation. Regeneration or remodeling of the Achilles tendon can be non-invasively detected and monitored in diffusion tensor imaging. Assessment of healing is possible using T2-mapping while evaluating the tendon vascularization in intravoxel incoherent motion MRI.
Keywords: Achilles tendon; Achilles tendon xanthoma; MRI; Spondyloarthropathy; Tendon.
© 2021 The Author(s).
Conflict of interest statement
The Swedish Ethics Committee approved the study and waived the need for informed consent (2020-06177). This project did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors declare that there is no conflict of interest.
Figures
Similar articles
-
Magnetic resonance imaging in chronic Achilles tendinopathy.Acta Radiol Suppl (Stockholm). 2004 Sep;(432):1-45. doi: 10.1080/03655950410009742. Acta Radiol Suppl (Stockholm). 2004. PMID: 15586844
-
Intravoxel incoherent motion (IVIM) imaging in human achilles tendon.J Magn Reson Imaging. 2018 Dec;48(6):1690-1699. doi: 10.1002/jmri.26182. Epub 2018 May 9. J Magn Reson Imaging. 2018. PMID: 29741808
-
Ultrasound detection of heel enthesitis: a comparison with magnetic resonance imaging.J Rheumatol. 2003 Apr;30(4):774-8. J Rheumatol. 2003. PMID: 12672198
-
MRI of the Achilles tendon - a comprehensive pictorial review. Part two.Eur J Radiol Open. 2021 Mar 27;8:100343. doi: 10.1016/j.ejro.2021.100343. eCollection 2021. Eur J Radiol Open. 2021. PMID: 33850972 Free PMC article. Review.
-
Diagnostic accuracy of ultrasound and MRI for Achilles tendon xanthoma in people with familial hypercholesterolemia: A systematic review.J Clin Lipidol. 2019 Jan-Feb;13(1):40-48. doi: 10.1016/j.jacl.2018.10.013. Epub 2018 Nov 7. J Clin Lipidol. 2019. PMID: 30503304
Cited by
-
Insertional Achilles tendinopathy: A radiographic cross-sectional comparison between symptomatic and asymptomatic heel of 71 patients.Eur J Radiol Open. 2024 May 10;12:100568. doi: 10.1016/j.ejro.2024.100568. eCollection 2024 Jun. Eur J Radiol Open. 2024. PMID: 38765668 Free PMC article.
-
Ultrasonographic insights into the complex anatomy and biomechanical dynamics of the Achilles tendon and its fascicles: a pictorial essay.J Ultrasound. 2025 Jun;28(2):505-516. doi: 10.1007/s40477-025-00987-z. Epub 2025 Feb 3. J Ultrasound. 2025. PMID: 39899233 Free PMC article.
-
Outcomes After Extracorporeal Shockwave Therapy for Chronic Noninsertional Achilles Tendinopathy Compared With Chronic Insertional Achilles Tendinopathy: A Retrospective Review.Orthop J Sports Med. 2024 Sep 4;12(9):23259671241265330. doi: 10.1177/23259671241265330. eCollection 2024 Sep. Orthop J Sports Med. 2024. PMID: 39247530 Free PMC article.
-
Minimally invasive excision and reconstruction of Achilles tendon xanthoma using free autologous semitendinosus tendon transfer: a surgical technique.J Orthop Surg Res. 2023 Apr 4;18(1):274. doi: 10.1186/s13018-023-03757-x. J Orthop Surg Res. 2023. PMID: 37013640 Free PMC article.
-
An in-depth study on the magnetic resonance imaging characteristics of tendon rupture in sports injuries and its correlation with patients' clinical symptoms.Eur J Transl Myol. 2024 Apr 12;34(2):12424. doi: 10.4081/ejtm.2024.12424. Eur J Transl Myol. 2024. PMID: 38618892 Free PMC article.
References
-
- Szaro P., Witkowski G., Śmigielski R., Krajewski P., Ciszek B. Fascicles of the adult human Achilles tendon – an anatomical study. Ann. Anat. - Anat. Anzeiger. 2009;191(6):586–593. - PubMed
-
- Pękala P.A., Henry B.M., Ochała A., Kopacz P., Tatoń G., Młyniec A., Walocha J.A., Tomaszewski K.A. The twisted structure of the Achilles tendon unraveled: a detailed quantitative and qualitative anatomical investigation. Scand. J. Med. Sci. Sports. 2017;27(12):1705–1715. - PubMed
-
- Abelkis E., Willekens I., Boulet C., Buls N., Provyn S., De Smet A., De Maeseneer M. Pseudo-tear appearance of the Achilles tendon on MR imaging in normal volunteers. Surg. Radiol. Anat. 2020;43(1):73–77. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
