

Frontotemporal dementia subtypes based on behavioral inhibition deficits
- PMID: 33851004
- PMCID: PMC8022767
- DOI: 10.1002/dad2.12178
Frontotemporal dementia subtypes based on behavioral inhibition deficits
Abstract
Introduction: We aimed to investigate phenotypic heterogeneity in the behavioral variant of frontotemporal dementia (bvFTD) through assessment of inhibition deficits.
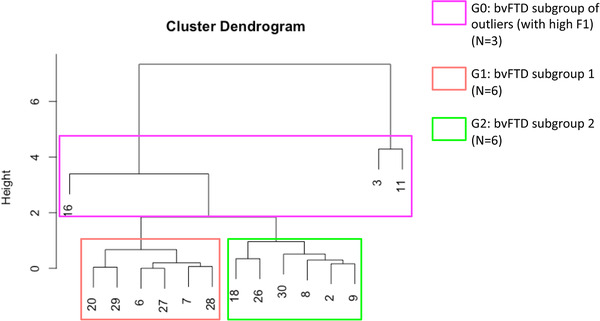
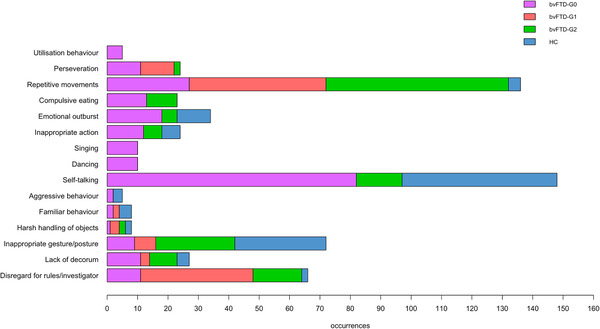
Methods: We assessed occurrences of 16 behavioral inhibition deficits from video recordings of 15 bvFTD patients (early stage) and 15 healthy controls (HC) in an ecological setting. We extracted dimensions of inhibition deficit and analyzed their correlations with cognitive and clinical measures. Using these dimensions, we isolated patient clusters whose atrophy patterns were explored.
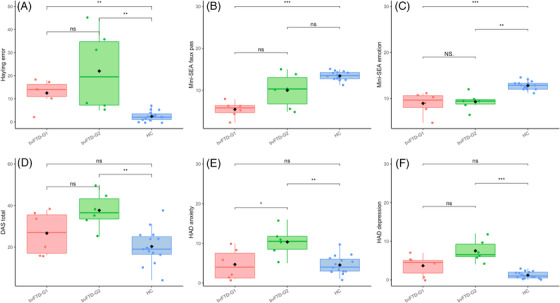
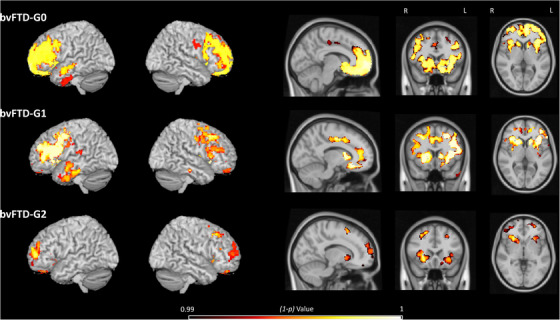
Results: After identifying two patterns of inhibition deficit (compulsive automatic behaviors and socially unconventional behaviors), we isolated three behavioral clusters with distinct atrophy patterns. BvFTD-G0 (N = 3), an outlier group, showed severe behavioral disturbances and more severe ventromedial prefrontal cortex/orbitofrontal cortex atrophy. Compared to bvFTD-G1 (N = 6), bvFTD-G2 (N = 6) presented higher anxiety and depression along with less diffuse atrophy especially in midline regions.
Discussion: Identifying clinico-anatomical profiles through behavior observation could help to stratify bvFTD patients for adapted treatments.
Keywords: compulsivity; disinhibition; ecological design; frontotemporal dementia; gray matter atrophy; subtypes.
© 2021 The Authors. Alzheimer's & Dementia: Diagnosis, Assessment & Disease Monitoring published by Wiley Periodicals, LLC on behalf of Alzheimer's Association.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Harnishfeger KK. The development of cognitive inhibition: theories, definitions, and research evidence. In: Dempster FN & Brainerd CJ Eds. Interference and Inhibition in Cognition. San Diego, CA: Academic Press; 1995.
-
- Paholpak P, Carr AR, Barsuglia JP, et al. Person‐based versus generalized impulsivity disinhibition in frontotemporal dementia and Alzheimer disease. J Geriatr Psychiatry Neurol. 2016;29:344‐351. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical