

Structural Covariance of Cortical Gyrification at Illness Onset in Treatment Resistance: A Longitudinal Study of First-Episode Psychoses
- PMID: 33851203
- PMCID: PMC8530394
- DOI: 10.1093/schbul/sbab035
Structural Covariance of Cortical Gyrification at Illness Onset in Treatment Resistance: A Longitudinal Study of First-Episode Psychoses
Abstract
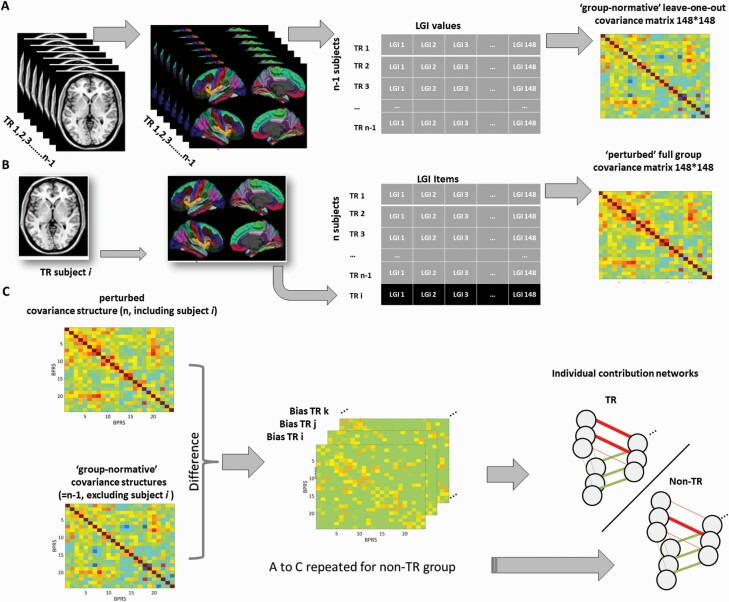
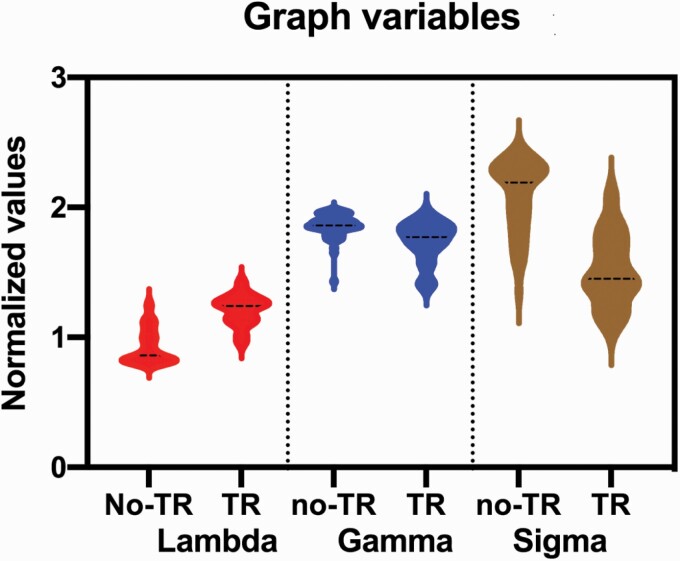
Treatment resistance (TR) in patients with first-episode psychosis (FEP) is a major cause of disability and functional impairment, yet mechanisms underlying this severe disorder are poorly understood. As one view is that TR has neurodevelopmental roots, we investigated whether its emergence relates to disruptions in synchronized cortical maturation quantified using gyrification-based connectomes. Seventy patients with FEP evaluated at their first presentation to psychiatric services were followed up using clinical records for 4 years; of these, 17 (24.3%) met the definition of TR and 53 (75.7%) remained non-TR at 4 years. Structural MRI images were obtained within 5 weeks from first exposure to antipsychotics. Local gyrification indices were computed for 148 contiguous cortical regions using FreeSurfer; each subject's contribution to group-based structural covariance was quantified using a jack-knife procedure, providing a single deviation matrix for each subject. The latter was used to derive topological properties that were compared between TR and non-TR patients using a Functional Data Analysis approach. Compared to the non-TR patients, TR patients showed a significant reduction in small-worldness (Hedges's g = 2.09, P < .001) and a reduced clustering coefficient (Hedges's g = 1.07, P < .001) with increased length (Hedges's g = -2.17, P < .001), indicating a disruption in the organizing principles of cortical folding. The positive symptom burden was higher in patients with more pronounced small-worldness (r = .41, P = .001) across the entire sample. The trajectory of synchronized cortical development inferred from baseline MRI-based structural covariance highlights the possibility of identifying patients at high-risk of TR prospectively, based on individualized gyrification-based connectomes.
Keywords: MRI; clozapine; first-episode psychosis; gyrification; longitudinal; schizophrenia; treatment-resistant.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Maryland Psychiatric Research Center.All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Elkis H, Buckley PF. Treatment-resistant schizophrenia. Psychiatr Clin North Am. 2016;39(2):239–265. - PubMed
-
- Kane J, Honigfeld G, Singer J, Meltzer H. Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Arch Gen Psychiatry. 1988;45(9):789–796. - PubMed
-
- Demjaha A, Egerton A, Murray RM, et al. Antipsychotic treatment resistance in schizophrenia associated with elevated glutamate levels but normal dopamine function. Biol Psychiatry. 2014;75(5):e11–e13. - PubMed
-
- Lally J, Ajnakina O, Di Forti M, et al. Two distinct patterns of treatment resistance: clinical predictors of treatment resistance in first-episode schizophrenia spectrum psychoses. Psychol Med. 2016;8:1–10. - PubMed
-
- Ajnakina O, Agbedjro D, Lally J, et al. Predicting onset of early- and late-treatment resistance in first-episode schizophrenia patients using advanced shrinkage statistical methods in a small sample. Psychiatry Res. 2020;294:113527. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
